Arterial endofibrosis is an unusual condition, but an important one to keep in mind as a differential diagnosis, especially in the case of cyclists. When an athlete bends forward and exercises(say like cyclists), it can put pressure on and/or cause a kink in the arteries supplying the working muscles of the leg with oxygen, sugars and so forth. The artery affected is usually one of the external iliac arteries which supply the majority of blood to each leg, from the heart.
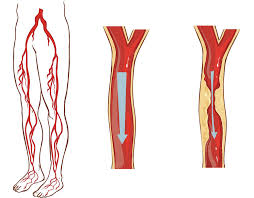
The theory is that the longer time spent bending forward and exercising, the more the artery can be kinked and irritated. Over time, the body responds to this irritation by making the artery harder, thereby reducing the irritation to the artery (a good outcome), but this hardening also reduces the blood supply to the leg when exercising (a bad outcome for bike racers).
With Arterial endofibrosis the patient typically complains of weakness and cramping, ‘bursting’ or aching pain of a single leg only during heavy efforts on the bike. They can’t ride through it, and in fact, the the harder they try, the worse it gets. The onset is usually slow, over months, but extremely consistent. Always with increasing intensity comes decreasing strength.
The patient may get treated by a number of therapists often misdiagnosing the condition, and diagnosing some other exotic sounding condition instead. One thing remains constant though; the symptoms persist. A simple, but not always conclusive test that doctors perform is to exercise the patient, then take their blood pressure at their arm and at their ankle. In a normal patient these two measurements will be the same or similar. In a patient with the problem, the blood pressure in the ankle of the effected leg will be lower (because it is getting less blood).
More invasive tests may follow. Treatment to correct the condition involves surgery. Often it is difficult to confirm the condition with absolute certainty. This is important because the surgery carries risk, so you really want to be as sure as possible. Surgery involves cutting out the kinked bit and sewing in another bit of vein from your leg instead, referred to as a ”patch”. Because a vein is a bit ‘flimsier’ than an artery, it bends a bit better. An artery has a muscular wall – which is why it pulses, making a patch using a piece of artery less suitable. Also you can ‘spare’ a bit of vein more than you can spare artery, and as a rule arteries run deep and are harder to harvest.
Return to cycling needs to be managed carefully post surgery, and has to be done under close medical supervision. However, the cyclist can eventually resume normal training/competition etc.
For more information see this video
Physiotherapists in Tralee. Open early until late. Phone 086-7700191.