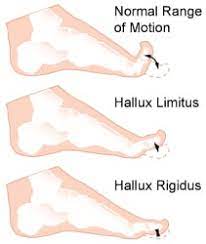
Big toe joint arthritis (otherwise known as Hallux Rigidus) is a form of degenerative arthritis. In this condition, surfaces of the joints in the big toe begin to wear away and extra bone can also develop in the form of bone spurs or osteophytes. This limits the movement of the joint. The big toe needs to bend significantly when stepping off. Consequently, arthritis in this joint can greatly affect walking, running etc.
Hallux Rigidus is a condition that tends to get worse over time. In it’s earlier stages, it may be referred to as Hallux Limitus, which is where there is limited movement of the big toe joint. With progression, Hallux Rigidus develops which can result in stiffness developing in the big toe joint and there may also be swelling.
To compensate for pain in the big toe joint, people with Hallux Rigidus tend to adjust their walking pattern which can also result in knee, hip or lower back pain. There is often difficulty finding shoes that fit properly shoes due to pain and/or inflammation in the joint. Early diagnosis can be made by physical examination and x-ray. Early treatment gives the best chance of avoiding surgery.
What causes Hallux Rigidus?
The big toe joint is designed to bear a considerable amount of stress during walking. However faulty biomechanics or structural abnormalities such as flat feet can stop the big toe from bending normally, and eventually lead to the development of osteoarthritis in the big toe joint. Other factors that can increase the risk of developing this condition include genetics (eg, having a certain foot type), injury to the big toe , other inflammatory diseases, and working in a job that places excessive stress on the big toe joint .
Treatment
In cases of Hallux Rigidus, certain types of footwear and orthotics may be recommended to reduce pressure and motion on the big toe. Custom orthotics that conform very closely to the arch of the foot are most effective in improving big toe joint function. These orthotics may incorporate something like a 3mm kinetic wedge in combination with a built in forefoot posting to take the pressure off the big toe joint. Ice and anti-inflammatory medication can also be used to reduce inflammation and pain. If it does not respond to conservative treatment, surgery may be recommended as a last resort in more severe cases.
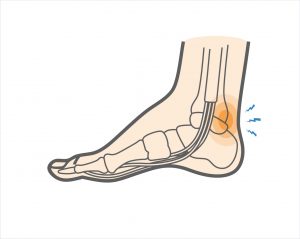
Posterior ankle impingement is a condition characterised by tissue damage at the back of
the ankle joint due to compression of these structures. This occurs when the foot and ankle
are pointed maximally away from the body (plantarflexion – figure 1. ). It may occur when
compressive forces are too repetitive and/or too forceful. This can occurs in the presence of
ankle swelling or bony anomalies, such as additional bone, a condition known as an “os
trigonum”. Posterior ankle impingement is most commonly found in gymnasts, ballet
dancers, and footballers, because they regularly maximally plantarflex their ankles during
their activities. The condition can also occur due to inadequate rehabilitation of an acute
ankle injury (ie. ankle sprain).
Mechanism of Injury
Posterior ankle impingement may develop due to an acute traumatic plantar hyperflexion
event, such as an ankle sprain. It may also occur as a result of repetitive low-grade trauma
associated with plantar hyperflexion, say like in case of a female ballet dancer. It is
important to differentiate between these two, because the latter, that is posterior
impingement from overuse, has a better prognosis.
The anatomy of the posterior ankle is a key factor in the occurrence of posterior
impingement syndrome . The more common causes of the condition are osseous in nature,
such as the os trigonum, an elongated posterolateral tubercle of the talus (known as
Stieda’s process), a downward sloping posterior lip of the tibia, an osteophyte from the
posterior distal tibia , or a prominent posterior process of the calcaneus. However, posterior
impingement can also be soft tissue related, as with a thickened posterior joint capsule ,
post-traumatic scar tissue, post-traumatic calcifications of the posterior joint capsule, or
loose bodies in the posterior part of the ankle joint. Symptoms for all of these conditions
relate to physical impingement of osseous or soft tissue structures, resulting in painful
limitation of the full range of ankle movement.
The most common cause ''os trigonum'' is an extra (accessory) bone that sometimes
develops behind the ankle bone (talus). The mineralized os trigonum appears between the
ages of 7 and 13 years and usually fuses with the talus within 1 year, forming the trigonal
(Stieda) process. It may remain as a separate ossicle in 7-14% of patients, and is often
bilateral(in both ankles). An os trigonum can be a focus of osseous abutment against other
structures. Pain can also be caused by disruption of the cartilaginous synchondrosis
between the os trigonum and the lateral talar tubercle as a result of repetitive microtrauma
and chronic inflammation.
In the case of soft tissue impingement it usually results from scarring and fibrosis associated
with synovial, capsular, or ligamentous injury ie. bad ankle sprain. It is thought that this
type of manifestation usually usually occurs when a significant soft-tissue component
forms. The soft-tissue component can consist of synovial thickening throughout the
posterior capsule or be more focal, involving the posterior intermalleolar or talofibular ligament. The flexor hallucis longus tendon runs in the groove between the lateral and
medial processes of the talus and can also be injured in posterior impingement, resulting in
tenosynovitis.
Signs and symptoms
Patients who have posterior impingement complain of chronic deep posterior ankle pain
worsened by forced plantar flexion or push-off forces as occur during activities such as
ballet dancing, jumping, or running downhill. In some patients, forced dorsiflexion(opposite
to plantarflexion) is also painful. Physical examination reveals pain on palpation over the posterolateral talar process, which is located along the posterolateral aspect of the ankle between the Achilles and peroneal
tendons . Passive forced plantar flexion results in pain and often a grinding
sensation as the posterolateral talar process is entrapped between the posterior tibia and
calcaneus.
Diagnosis of posterior ankle impingement
A thorough examination by an experienced practitioner may be all that is necessary to
diagnose posterior ankle impingement. Further investigations such as an X-ray, MRI, CT scan
or Ultrasound may help confirm diagnosis.
Physiotherapist in Tralee, Co. Kerry………..Phone 0867700191 to make an appointment or discuss your condition.
Suboccipital-Muscles-of-the-Neck
Suboccipital Muscles & Trigger Point Pain
Suboccipital muscles (see image) are a group of four muscles located on each side of the upper cervical spines, just below the base of the skull. The muscles connect the base of the skull with the top two vertebrae (C1 and C2) of the neck.
Poor posture in general especially with the increased use of portable electronic devices, which include mobile phones, laptops, and tablets has increased the prevalence of neck pain in both children and adults. Increased screen time on these devices is not only correlated with depression, sleep interruption, and poor food choices, but also rising rates of neck pain, especially in adolescents and young adults. This form of neck pain, including dysfunction of C1 and altered mechanics of the cervical spine due to poor posture, can also lead to headaches. Reading in bed is also a big offender. Any position where your head and neck are positioned forward and in a stationary position for long periods on time increases the likelihood of postural related spinal issues(ie. kyphosis, discogenic disorders etc.), neck pain and headaches.
These suboccipital muscles play an important role in controlling movements of your head and neck, providing sensory input and are also linked closely to vestibular and balance functions. However, when the suboccipital muscles become tightened, the following symptoms may occur. These could include:
Stiff neck
Neck pain
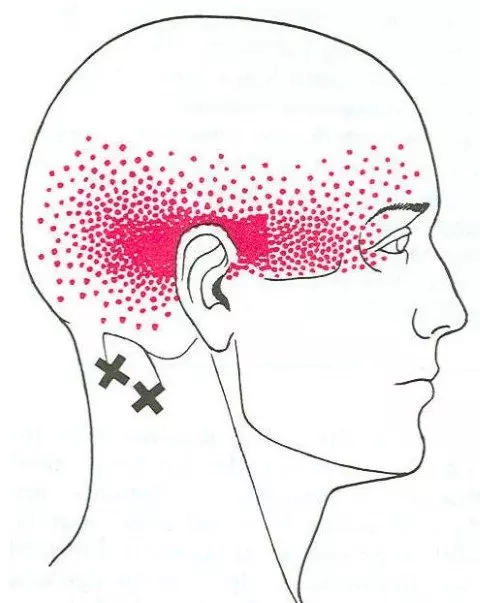
Headaches with a band of pain on the side of the head that extends from the back of the head to the eye as a result of active trigger points. This type of pain feels deep in the head, and often it is difficult to describe.
Messages sent to the brain may be altered, which is also why sometimes headache sufferers may also experience sensory symptoms, including dizziness and visual disturbances.
Physiotherapy Treatment
Treatment includes deep tissue work, trigger point release, manipulation, mobilisation, postural education and a rehabilitation program.
Overview of Shoulder Impingement by Physiotherapist in Tralee
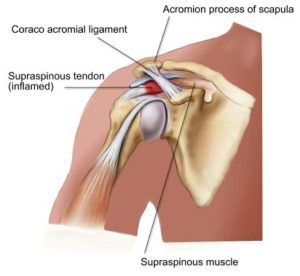
Shoulder impingement is a very common cause of shoulder pain, where a supraspinatus tendon inside the shoulder rubs or catches on nearby tissue and/or bone(acromium) as you lift your arm. Your shoulder is made up of several joints, muscles and tendons which allow the great range of motion in your arm. There are three bones in the shoulder joint: your upper arm bone, your shoulder blade, and your collarbone . Your arm is kept in your shoulder socket by your rotator cuff muscles, along with ligaments and the joint capsule which envelopes the shoulder. There is a lubricating sac called a bursa between the supraspinatus muscle of the rotator cuff where the supraspinatus travels under the bone on top of your shoulder (acromion). The bursa allows the supraspinatus tendon to glide freely under the acromium when you move your arm. When the bursa becomes swollen and inflamed, the condition is called bursitis and is one cause of shoulder impingement. Bone spurs within the shoulder joint can also contribute to impingement, as can forward curving shoulders due to years of bad posture. Sometimes due to impingement and/or bone spurs the supraspinatus muscle or tendon can tear. It can also happen during an accident like a shoulder dislocation or falling on a shoulder etc. Those who do repetitive lifting or overhead activities using the arm, such as paper hanging, construction, or painting are also susceptible.
Symptoms of shoulder impingement
You may have pain and stiffness when you lift your arm. There may also be pain when the arm is lowered from an elevated position. Early symptoms may be mild. Patients frequently do not seek treatment at an early stage. These symptoms may include:
Minor pain that is present both with activity and at rest
Pain radiating from the front of the shoulder to the side of the arm
Sudden pain with lifting and reaching movements
Athletes in overhead sports may have pain when throwing or serving a tennis ball
As the problem progresses, the symptoms increase:
Pain at night
Loss of strength and motion
Difficulty doing activities that place the arm behind the back, such as buttoning or zippering
If the pain comes on suddenly, the shoulder may be severely tender. All movement may be limited and painful.
Imaging Tests
Other tests which may help your doctor confirm your diagnosis include:
X-rays. Becauses x-rays do not show the soft tissues of your shoulder like the rotator cuff, plain x-rays of a shoulder with rotator cuff pain are usually normal or may show a small bone spur. A special x-ray view, called an “outlet view,” sometimes will show a small bone spur on the front edge of the acromion.
Magnetic resonance imaging (MRI) and ultrasound. These studies can create better images of soft tissues like the rotator cuff tendons. They can show fluid or inflammation in the bursa and rotator cuff. In some cases, partial tearing of the rotator cuff will be seen.
Treatment
The goal of treatment is to reduce pain and restore function. In planning your treatment, your doctor will consider your age, activity level, and general health.
TreatmentIn cases where there is a tear in the supraspinatus muscle or tendon, conservative treatment such as rest, physio etc rarely works. In milder cases rest along with rehab and correction of postural problems in the shoulder may work.Rest. Your doctor may suggest rest and activity modification, such as avoiding overhead activities.
Non-steroidal anti-inflammatory medicines. Drugs like ibuprofen and naproxen reduce pain and swelling in mild cases.
Physical therapy. A physical therapist will initially focus on restoring normal motion to your shoulder. Stretching exercises to improve range of motion are very helpful. If you have difficulty reaching behind your back, you may have developed tightness of the posterior capsule of the shoulder (capsule refers to the inner lining of the shoulder and posterior refers to the back of the shoulder). Specific stretching of the posterior capsule can be very effective in relieving pain in the shoulder.
Once your pain is improving, your therapist can start you on a strengthening program for the rotator cuff muscles.
Steroid injection. Cortisone is a very effective anti-inflammatory medicine. Injecting it into the bursa beneath the acromion can relieve pain and reduce symptoms dramatically if the sole cause of the impingement is bursitis.
Surgical Treatment
When nonsurgical treatment does not relieve pain, your doctor may reoved. This is also known as a subacromial decompression. These procedures can be performed using either an arthroscopic or open technique.
Arthroscopic technique. In arthroscopy, thin surgical instruments are inserted into two or three small puncture wounds around your shoulder. Your doctor examines your shoulder through a fiberoptic scope connected to a television camera. He or she guides the small instruments using a video monitor, and removes bone and soft tissue. In most cases, the front edge of the acromion is removed along with some of the bursal tissue.
Your surgeon may also treat other conditions present in the shoulder at the time of surgery. These can include arthritis between the clavicle (collarbone) and the acromion (acromioclavicular arthritis), inflammation of the biceps tendon (biceps tendonitis), or a partial rotator cuff tear.
Open surgical technique. In open surgery, your doctor will make a small incision in the front of your shoulder. This allows your doctor to see the acromion and rotator cuff directly.
Rehabilitation. After surgery, your arm may be placed in a sling for a short period of time. This allows for early healing. As soon as your comfort allows, your doctor will remove the sling to begin exercise and use of the arm.
The temporomandibular joint works as a combination of hinge and sliding actions. It connects the jawbone to the skull on each side of the face. The parts of the bones that interact in the joint are covered with cartilage and are separated by a small shock-absorbing disk, which normally keeps the movement smooth. Temporomandibular joint disorder (TMJD) can cause pain in your jaw joint and in the muscles that control jaw movement.
Symptoms
Pain in one or both of the temporomandibular joints
Difficulty or pain chewing
Locking of the joint, making it difficult to open or close your mouth
Clicking sound or grating sensation when you open your mouth or chew
Causes of Temporomandibular Joint Disorder
Painful TMJ disorders can occur if:
The disk erodes or moves out of its proper alignment
The joint’s cartilage is damaged by arthritis
The joint is damaged by a blow or other impact
In many cases, however, the cause of TMJ disorders is unclear.
Treatment of Temporomandibular Joint Disorder
In some cases, the symptoms of TMJ disorders may go away without treatment. Some of the following may also help.
Medications
Pain relievers and anti-inflammatories. These can help relieve pain and inflammation.
Muscle relaxants. These can help relax the jaw muscles.
Therapies
Nondrug therapies for TMJ disorders include:
Oral splints or mouth guards. These devices worn at night while sleeping can help prevent grinding of the teeth.
Physical therapy. Deep tissue massage work on neck and jaw muscles can be beneficial along with certain rehabilitation exercises.
Education. Education can help you understand the factors and behaviors that may aggravate your pain, so you can avoid them. Examples include teeth clenching or grinding, eating foods where you have to open the jaw wide like apples and burgers.
When conservative treatments fail, the following may be considered:
Arthrocentesis. This is a minimally invasive procedure that involves the insertion of small needles into the joint so that fluid can be irrigated through the joint to remove debris and inflammatory byproducts.
Injections. In some people, corticosteroid injections into the joint may be helpful. Infrequently, injecting botulinum toxin type A (Botox, others) into the jaw muscles used for chewing may relieve pain associated with TMJ disorders.
TMJ arthroscopy. A small thin tube is placed into the joint space, an arthroscope is then inserted and small surgical instruments are used for surgery. TMJ arthroscopy has fewer risks and complications than open-joint surgery does, but it has some limitations as well.
Modified condylotomy. Modified condylotomy addresses the TMJ indirectly, with surgery on the mandible, but not in the joint itself. It may be helpful for treatment of pain and if locking is experienced.
Open-joint surgery. If your jaw pain does not resolve with more-conservative treatments and it appears to be caused by a structural problem in the joint, your doctor or dentist may suggest open-joint surgery (arthrotomy) to repair or replace the joint. However, open-joint surgery involves more risks than other procedures do.
Check out our website and feel free to contact us to discuss your condition or to set up an appointment.
Patella
Patella Dislocation – knee Injury
The patella, or kneecap lies in front of the knee joint. It is attached to the quadriceps muscle via the quadriceps tendon and acts to increase the leverage from this muscle group when straightening the knee. The patella glides up and down virtically within a groove called the patello-femoral groove at the front of the thigh bone(femur) during knee bending. Patella dislocation occurs when the patella moves outside of this groove. The patella may also sublux rather than fully dislocate, meaning it only moves partially out of position. These injuries usually occurs as a result of an acute blow to or as a result of a twisting action on the knee. In most cases the patella will relocate into the patello-femoral groove on straightening of the knee. This, however is usually extremely painful. Risk factors which make a patella dislocation more likely are 1. insufficient quadriceps strength especially on the inside of the knee, 2. over pronation of the feet , and 3. an increased Q angle of the knee.
The vastus medialis obliqus muscle (VMO) is part of the quadriceps muscle group on the inside of the thigh, and is responsible for maintaining the stability of the patella towards the inside of the knee. If the VMO isn’t strong enough, the patella is much more susceptible to dislocation.
Over pronation of the feet is where the feet roll in(collapse in slightly on the flattened arch with the toes turning outwards) when running. This causes torsion at the knee, leaving the patella susceptible to moving outwards as the quadriceps contract.
The Q-angle of the knee is theangleformed by linesrepresentingthepull of the quadricepsmuscleandtheaxis of thepatellartendon. People with an increased Q ankle are often termed knock kneed. This angle when too large increases the risk of patellar dislocation.
Treatment of patella dislocation
Apply RICE(rest, ice, compression and elevation) principles to the injured knee . Ice can be applied for 10 to 15 minutes every hour initially reducing to 2 or 3 times a days as swelling and symptoms reduce. Also medications like non steroidal anti-inflammatories (NSAIDs), analgesics, pain killers etc. would be beneficial, in order to manage both the inflammation and the pain .
Rest from any sporting activities and seek medical advice. An athlete who has had one episode of patella dislocation is often susceptible to another. The knee may need to be immobilized for 2-3 weeks initially. A knee support can provide protection for the joint initially during rehab. Patella stabilizing braces have been specifically designed to provide support for the knee cap.
Quadriceps strengthening is initiated during this phase. These should be in the form of static exercises. Quadriceps electrical stimulation is an option for muscle reeducation if the patient has difficulty activating the muscle secondary to pain. Electrical stimulation may also play a role in the management of knee joint effusion. When swelling, inflammation has subsided, the patient may progress to the recovery phase of rehabilitation.
When the acute symptoms settle down a full knee strengthening rehabilitation program is required to help avoid future recurrence. Specifically exercises for the VMO muscle on the inside of the quadriceps are important, but overall quadriceps strengthening is also beneficial . The VMO is an important medial stabilizer of the patella. The prevailing theory has been that lateral patellar tracking is associated with VMO weakness. However, research has been inconclusive for VMO weakness as a direct causative mechanism of lateral patellar tracking(patellar subluxation/dislocation). Recent findings have shown that general quadriceps strengthening has demonstrated reductions in lateral tracking irrespective of the mechanism. Therapy should also include a protocol for hamstring muscle stretching. Tight hamstring muscles functionally counteract their agonist group, the quadriceps.
Any physical therapy program for patellofemoral problems must address any tightness or reduced flexibility in the quadriceps, hamstrings, hip abductors, iliotibial band and calf muscles.
Medial patellar gliding exercises may loosen lateral retinacular tightness in this stage. Medial patellar gliding exercises are performed with the leg extended. The patient manually pushes the patella medially and holds for a count of 10 seconds.
An important concept in the rehabilitation of patellar dislocation and patellofemoral pain is knee flexion. Initially, any activity that requires greater than 40-45° of knee flexion causes symptoms. Initial rehabilitation programs start with the isometric open kinetic chain . Early rehabilitation programs should limit all activities that require quadriceps firing with the knee flexed greater than 45°.
Once isometric open kinetic chain exercises are tolerated without discomfort, the rehabilitation program advances to closed kinetic chain exercises (eg, mini squats, lunges, stair climbing). The rectus femoris, VMO, and VL are all strengthened by the mini squats (repetitions and sets modified to the tolerance of the patient).
Important goals are to restore ”range of movement” in the joint, mobilize soft tissues, and strengthen the surrounding musculature. Lunges and bike riding allow strengthening through a controlled ”range of movement”. Once pain has resolved sufficiently to complete daily activity requirements without exacerbations, the patient can advance to the final phase of rehabilitation.
Advanced rehabilitation programs progress to jogging, running, plyometrics, and sport-specific exercises. Patients must be monitored and must always follow proper technique, as well as learn to properly fire the VMO.
Sometimes Surgery is needed. Most surgeons agree, if the kneecap dislocates multiple times, then surgery should be considered. When the kneecap dislocates, it is possible to damage the cartilage in the knee, leading to an increased risk of knee arthritis. When multiple dislocations occur, patellar stabilization surgery should be considered. While dislocations of the patella can occur after surgery, they are much less common.
Morton’s foot and pyridoxal 5′-phosphate deficiency: genetically linked traits.
I came across an extremely interesting article lately regarding Morton’s foot and vitamin B6 deficiency. A lot of what I say in the article comes from scientifically published research referenced at the end of the article. Apologies if some of it is a bit technical. I have tried to simplify it while keeping the content intact.
What is Morton’s foot?
A Morton’s foot also called Morton’s toe, is a condition characterized by a longer second toe.
Pathophysiology
Morton’s Toe will cause an individual to have abnormal or over pronation. It is this pronation that is the ultimate cause or contributing factor to most of the problems not only of the foot but also of the whole body.
Normal Pronation is a series of motions the foot must have, so that it can absorb the shock of meeting the ground. It must be able to do this, in order to adapt and adjust to the new walking surfaces it has just met. This adjustment should only last a fraction of a second to allow the foot to slow down; absorb the shock of your body weight in order to adjust and adapt to the walking surface. If this adjustments last longer, the foot will then begin to abnormally pronate and to correct itself. This is the start of a “chain reaction” that puts the foot under a lot of abnormal stress and strain, causing Bunions, Heel Spurs, plantar fasciitis, Corns, Callouses, ingrown toenails and numerous other foot problems.
Vitamin B6 deficiency
Vitamin B6 is an essential vitamin needed for many chemical reactions in the human body. It exists as several active forms but pyridoxal 5′-phosphate (PLP) is the phosphorylated form needed for transamination, deamination, and decarboxylation. PLP is important in the production of neurotransmitters, acts as a Schiff base and is essential in the metabolism of homocysteine, a toxic amino acid involved in cardiovascular disease, stroke, thrombotic and Alzheimer’s disease. Nichols and Gaiteri(2014) showed the connection between a deficit of pyridoxal 5′-phosphate and the physical foot deformity known as the Morton’s foot. Morton’s foot has been associated with fibromyalgia/myofascial pain syndrome. PLP deficiency also plays a role in impaired glucose tolerance and may play a much bigger role in the obesity, diabetes, fatty liver and metabolic syndrome. Without the Schiff-base of PLP acting as an electron sink, storing electrons and dispensing them in the mitochondria, free radical damage occurs.
Summary
To put this all very simply : Vitamin B6 is an essential vitamin needed for many chemical reactions that take place within the human body. This vitamin is obtained from your diet. The genetically linked condition of ”Morton’s toe” has been linked to the inability to convert Vitamin B6 into the active form pyridoxal 5′-phosphate needed for cetain chemical processes in the human body. This in turn can lead to conditions seen with vitamin B6 deficiency. Some of these conditions include:
Anemia
Skin/Hair/Nail problems
Depression/Anxiety
Nerve damage
Pain syndrome development
Systemic Inflammation
Circulation problems, including oxygen transport
Hormone Issues
Seizures
Do not take a B6 supplement, or “b-vitamin complex” and expect it to help. It won’t. You need the activated form of B6 called P5P. This is the only form that your body can use.
Reference:
Supplementation with PLP, L5-MTHF, B12 and trimethylglycine should be used in those patients with hyperhomocysteinemia and/or MTHFR gene mutation.(Trent W. Nichols, Christopher Gaiteri ,Published in Medical hypotheses2014, DOI:10.1016/j.mehy.2014.09.003).
When Back Pain Is A Symptom Rather Than A Condition
Back pain may sometimes be a symptom rather than a condition as such. A practitioner needs to always keep this at the back of their mind when treating or assessing somebody. Sometimes things need more investigation. A good physio will spot this early and refer you on quickly to your G.P. for further examination. It is always better to play it safe if in doubt. I always believe you should be seeing improvement in your condition from treatment to treatment. If there is no improvement after several treatments you need to be asking yourself a few questions i.e. Do I need to try a different physio or do I need to consult my doctor for a second opinion. Sometimes the proper treatment protocol for a condition is all that is needed for a swift recovery. The list below is not meant to be alarmist. It is more to emphasize the fact that continuous unrelenting back pain can be a symptom of something else going on within your body.
Below are examples of conditions/medications etc. that may have back pain as a side effect/symptom.
kidney stones – A kidney stone may not cause symptoms until it moves around within your kidney or passes into your ureter (the tube connecting the kidney and bladder). At that point, you may experience symptoms such as severe pain in your side and back below the ribs, or pain that radiates into the lower abdomen and groin.
Lupus is a long-term autoimmune disease in which the body’s immune system becomes hyperactive and attacks normal, healthy tissue. Symptoms include inflammation, swelling, and damage to the joints, skin, kidneys, blood, heart, and lungs. Lupus can cause neck and back pain, because muscles in these areas can become inflamed due to the lupus. Furthermore, the muscle pain syndrome ”fibromyalgia” can cause pain in these areas and is commonly associated with lupus.
Spinal arthritis/facet joint arthritis causes stiffness and back pain.
Cancers – A primary bone cancer tumor in the spine can cause back pain, as can a number of other cancers when they have metastasized(spread to other sites in the body), such as breast cancer, testicular cancer, colon cancer, and lung cancer. In fact, back pain is often the one of first symptoms that people with lung cancer notice before they are diagnosed. A tumor in the lungs can put pressure on the spine, or can affect the nerves around the chest wall and spine.
Spondylosis a painful condition of the spine resulting from the degeneration of the intervertebral discs.
Spondylitis is a condition resulting in inflammation within the joints of the spine. As the inflammation goes and healing takes place, bone grows out from both sides of the vertebrae and may join the two together, causing a stiffening known as ankylosis. The progressed condition is called ankylosing spondylitis. The cause is not yet known.
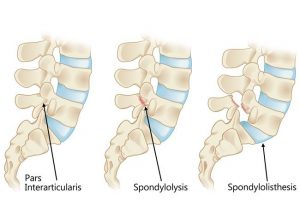
Spondylolisthesis is a slipping of vertebra that occurs, in most cases, at the base of the spine.
Spondylolysis is a defect or fracture of one or both wing-shaped parts of a vertebra, can result in vertebrae slipping backward, forward, or over a bone below.
Spondylosis, Spondylitis, Spondylolisthesis, Spondylolysis all have back pain as a symptom.
Fractures – Even a minor fracture along the spine can cause considerable back pain.
Statins – Statins are drugs that can help lower your cholesterol. One of the more severe side effect of statins is myotoxicity(having a toxic effect on muscle), in the form of myopathy(a disease of the muscle in which the muscle fibers do not function properly. This results in muscular weakness), myalgia(muscle pain), myositis(inflammation and degeneration of muscle tissue) or rhabdomyolysis(a condition in which damaged skeletal muscle breaks down). Currently, the only effective treatment of statin-induced myopathy is the discontinuation of statin use in patients affected by muscle aches, pains and elevated creatine kinase levels. Creatine kinase are the clinical measure of muscle damage (rhabdomyolysis).
Anticonvulsant drugs such those used in the treatment of conditions like epilepsy can cause changes in calcium and bone metabolism. This may in time lead to decreased bone mass and a risk of osteoporotic fractures in the spine which may also result in severe back pain. Two widely used antiepileptic drugs phenytoin and carbamazepine are recognized to have direct effects on bone cells.
Corticosteroids – Longterm use of corticosteroids increase the risk of compression fractures in the spine(back).
Neurological Compromise — A Red Flag
Neural compromise can result from spinal cord or cauda equina compression . Cauda equina compression usually results from a fracture, tumor, epidural hematoma, or abscess, and occasionally from a massive disk herniation. Paraplegia(impairment in motor or sensory function of the lower extremities), quadriplegia(paralysis caused by illness or injury that results in the partial or total loss of use of all four limbs and torso), or cauda equina deficit should trigger an aggressive search for the cause.
Cauda equina compression classically presents with back pain, bilateral sciatica(pain down the back of both legs), saddle anesthesia, and lower extremity weakness progressing to paraplegia, but in practice these symptoms are variably present and diagnosing the condition often requires a high degree of suspicion. Hyporeflexia(no reflexes) is typically a sign of cauda equina compression, while hyperreflexia(overresponsive reflexes), clonus(series of involuntary, rhythmic, muscular contractions and relaxations), and the Babinski sign(see below *) suggest spinal cord compression, requiring an evaluation of the cervical and thoracic spine. Cauda equina compression typically involves urinary retention; in contrast, cord compression typically causes incontinence. If either cauda equina or spinal cord compression is detected during an initial examination, an immediate more extensive evaluation is warranted. MRI is the study of choice.
*(The Babinski reflex occurs after the sole of the foot has been firmly stroked. The big toe then moves upward or toward the top surface of the foot. The other toes fan out. This reflex is normal in children up to 2 years old. It disappears as the child gets older. It may disappear as early as 12 months. When the Babinski reflex is present in a child older than 2 years or in an adult, it is often a sign of a central nervous system disorder. The central nervous system includes the brain and spinal cord.)
Spinal epidural hematoma
Spinal epidural hematoma is a rare but dramatic cause of paralysis in elderly patients. In most cases, there is no antecedent trauma. Lawton et al. (1995), in a series of 30 patients treated surgically for spinal epidural hematoma, found that 73% resulted from spine surgery, epidural catheterization, or anticoagulation therapy. Other possible causes of epidural hematoma include vascular malformations, angiomas, aneurysms, hypertension, and aspirin therapy. The same study found that the time from the first symptom to maximal neurologic deficit ranged from a few minutes to 4 days, with the average interval being nearly 13 hours.
Although painless onset has been reported, spinal epidural hematoma typically presents with acute pain at the level of the lesion, which is often rapidly followed by paraplegia(impairment in motor or sensory function of the lower extremities) or quadriplegia(is paralysis caused by illness or injury that results in the partial or total loss of use of all four limbs and torso), depending on the location of the hemorrhage. Sometimes the onset of pain is preceded by a sudden increase of venous pressure from coughing, sneezing, or straining at stool. Urinary retention often develops at an early stage.
Most lesions occur in the thoracic region(rib area of back) and extend into the cervicothoracic(upper back and neck) or the thoracolumbar(ribs to lower back area) area. The pain distribution may be radicular(affecting or relating to the root of a spinal nerve), mimicking a ruptured intervertebral disk.
Evaluation should be with MRI. Early recognition, MRI confirmation, and treatment should be accomplished as soon as possible. Recovery depends on the severity of the neurologic deficit and the duration of symptoms before treatment. Lawton et al.(1995), found that patients taken to surgery within 12 hours had better neurologic outcomes than patients with identical preoperative neurologic status whose surgery was delayed beyond 12 hours. Surgery should not be withheld because of advanced age or poor health: in 10 reported cases in which surgery was delayed, all patients died.
For more about treatments and opening times etc. click on our homepage
Everyone’s spine has curves, from your neck down to your lower back. These curves, which create the spine’s ”S” shape, are lordotic in shape in the neck and lower back, and kyphotic in shape for the upper back. They help your body 1. absorb shock, 2. support the weight of the head, 3. align your head over your pelvis, 4. stabilize and maintain its structure, 5. move and bend flexibly. When these curves are exaggerated through poor posture or hereditary conditions like scoliosis, spinal pain and problems can develop over time.
Kyphosis
Kyphosis is an exaggerated, forward rounding of the back. It can occur at any age but is more common in older people. Age-related kyphosis is often due to weakness in the spinal bones that causes them to compress or crack. Other types of kyphosis can appear in infants or teens due to malformation of the spine or wedging of the spinal bones over time. Mild kyphosis causes few problems. Severe kyphosis can cause pain and be disfigurment. Treatment for kyphosis depends on your age, and both the cause and the effects of the curvature.
Lordosis
Some curvature in the lower back is normal. However, if your curve arches too far inward, it’s called lordosis, or swayback. Lordosis can affect your lower back and/or neck. The condition can lead to excess pressure on the spine, causing pain and discomfort. It can affect your ability to move if it’s severe and left untreated. Treatment of lordosis depends on how serious the curve is and how you got lordosis. There’s little medical concern if your lower back curve reverses itself when you bend forward. You can probably manage your condition with physical therapy and daily exercises.
Scoliosis
Scoliosis is a medical condition in which a person’s spine curves sideways, usually in an “S” or “C” shape. In some, the degree of curvature remains stable, while in others, it increases over time. Mild scoliosis does not typically cause problems, however severe cases can interfere with breathing. The cause of most cases is unknown, but is believed to involve a combination of genetic and environmental factors. Diagnosis is confirmed by Xray. Treatment depends on the degree of curve, location, and cause.
Minor curves may simply be watched periodically. Treatments may include bracing or surgery in more severe cases. The brace must be fitted to the person and used daily until growing stops.Evidence that chiropractic manipulation dietary supplements, or exercises can prevent the condition from worsening is non existent. However, exercise is still recommended due to its other health benefits. Scoliosis occurs in about 3% of people. It most commonly occurs between the ages of 10 and 20. Girls typically are more severely affected than boys.
Bicipital tendonitis is a common cause of shoulder pain, often developing in people who perform repetitive, overhead movements. Biceps tendinitis develops over time, the pain being located at the front of the shoulder. The biceps muscle has two parts referred to as the long head and the short head. The tendon of the long head of the biceps is most commonly implicated with tendonitis. When this tendon is subjected to repetitive stresses, it can become irritated, swollen, and painful.This occurs where the tendon sits within the bicipital groove at the top of the humerus under the transverse ligament before it becomes part of the shoulder joint capsule.
Pain at this exact spot when pressed with a finger as the arm is rotated in and out while standing, is usually a fairly reliable test to confirm this condition. Imaging techniques such as MRI are typically not needed to diagnose biceps tendonitis.
Symptoms – Bicipital Tendonitis
Pain or tenderness in the front of the shoulder, which worsens with overhead lifting or activity.
Pain that moves down along the upper arm
An occasional snapping sound or sensation in the shoulder
Treatment – Bicipital Tendonitis
The initial goals of treatment for bicipital tendonitis are to reduce inflammation and swelling. Patients should restrict above shoulder height movements, reaching out with the affected arm and lifting. They should apply ice to the affected area for 10-15 minutes, 2-3 times daily for several days. Non-steroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, may help recovery. Probably the biggest aid to recovery is rest from the aggravating activity for several weeks. I often come across this condition in weight trainers who front press or incline bench press, the bar being too far out from their neck during pressing. It is also common in swimmers with poor technique or who ramp up their training distance/pace too quickly.
Physiotherapist Tralee : Phone 086-7700191 for an appointment, second opinion or to discuss your injury.
 Posterior ankle impingement is a condition characterised by tissue damage at the back of
Posterior ankle impingement is a condition characterised by tissue damage at the back of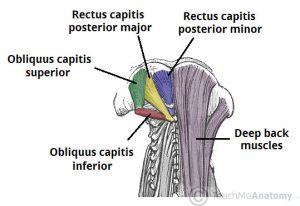
 Shoulder impingement is a very common cause of shoulder pain, where a supraspinatus tendon inside the shoulder rubs or catches on nearby tissue and/or bone(acromium) as you lift your arm.
Shoulder impingement is a very common cause of shoulder pain, where a supraspinatus tendon inside the shoulder rubs or catches on nearby tissue and/or bone(acromium) as you lift your arm. 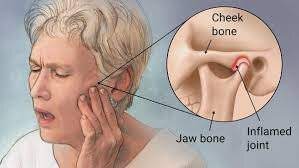 The temporomandibular joint works as a combination of hinge and sliding actions. It connects the jawbone to the skull on each side of the face. The parts of the bones that interact in the joint are covered with cartilage and are separated by a small shock-absorbing disk, which normally keeps the movement smooth. Temporomandibular joint disorder (TMJD) can cause pain in your jaw joint and in the muscles that control jaw movement.
The temporomandibular joint works as a combination of hinge and sliding actions. It connects the jawbone to the skull on each side of the face. The parts of the bones that interact in the joint are covered with cartilage and are separated by a small shock-absorbing disk, which normally keeps the movement smooth. Temporomandibular joint disorder (TMJD) can cause pain in your jaw joint and in the muscles that control jaw movement.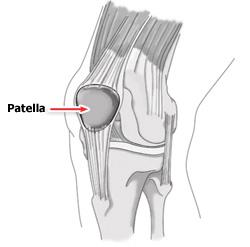

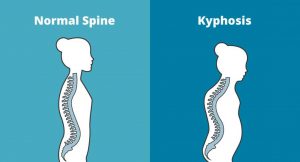 Kyphosis is an exaggerated, forward rounding of the back. It can occur at any age but is more common in older people. Age-related kyphosis is often due to weakness in the spinal bones that causes them to compress or crack. Other types of kyphosis can appear in infants or teens due to malformation of the spine or wedging of the spinal bones over time. Mild kyphosis causes few problems. Severe kyphosis can cause pain and be disfigurment. Treatment for kyphosis depends on your age, and both the cause and the effects of the curvature.
Kyphosis is an exaggerated, forward rounding of the back. It can occur at any age but is more common in older people. Age-related kyphosis is often due to weakness in the spinal bones that causes them to compress or crack. Other types of kyphosis can appear in infants or teens due to malformation of the spine or wedging of the spinal bones over time. Mild kyphosis causes few problems. Severe kyphosis can cause pain and be disfigurment. Treatment for kyphosis depends on your age, and both the cause and the effects of the curvature.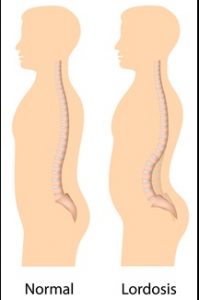 Some curvature in the lower back is normal. However, if your curve arches too far inward, it’s called lordosis, or swayback. Lordosis can affect your lower back and/or neck. The condition can lead to excess pressure on the spine, causing pain and discomfort. It can affect your ability to move if it’s severe and left untreated. Treatment of lordosis depends on how serious the curve is and how you got lordosis. There’s little medical concern if your lower back curve reverses itself when you bend forward. You can probably manage your condition with physical therapy and daily exercises.
Some curvature in the lower back is normal. However, if your curve arches too far inward, it’s called lordosis, or swayback. Lordosis can affect your lower back and/or neck. The condition can lead to excess pressure on the spine, causing pain and discomfort. It can affect your ability to move if it’s severe and left untreated. Treatment of lordosis depends on how serious the curve is and how you got lordosis. There’s little medical concern if your lower back curve reverses itself when you bend forward. You can probably manage your condition with physical therapy and daily exercises. Scoliosis is a medical condition in which a person’s spine curves sideways, usually in an “S” or “C” shape. In some, the degree of curvature remains stable, while in others, it increases over time. Mild scoliosis does not typically cause problems, however severe cases can interfere with breathing. The cause of most cases is unknown, but is believed to involve a combination of genetic and environmental factors. Diagnosis is confirmed by Xray. Treatment depends on the degree of curve, location, and cause.
Scoliosis is a medical condition in which a person’s spine curves sideways, usually in an “S” or “C” shape. In some, the degree of curvature remains stable, while in others, it increases over time. Mild scoliosis does not typically cause problems, however severe cases can interfere with breathing. The cause of most cases is unknown, but is believed to involve a combination of genetic and environmental factors. Diagnosis is confirmed by Xray. Treatment depends on the degree of curve, location, and cause.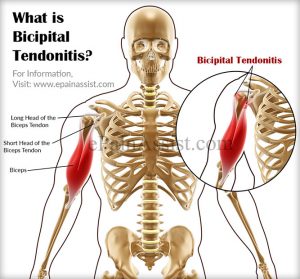 Bicipital tendonitis is a common cause of shoulder pain, often developing in people who perform repetitive, overhead movements. Biceps tendinitis develops over time, the pain being located at the front of the shoulder. The biceps muscle has two parts referred to as the long head and the short head. The tendon of the long head of the biceps is most commonly implicated with tendonitis. When this tendon is subjected to repetitive stresses, it can become irritated, swollen, and painful.This occurs where the tendon sits within the bicipital groove at the top of the humerus under the transverse ligament before it becomes part of the shoulder joint capsule.
Bicipital tendonitis is a common cause of shoulder pain, often developing in people who perform repetitive, overhead movements. Biceps tendinitis develops over time, the pain being located at the front of the shoulder. The biceps muscle has two parts referred to as the long head and the short head. The tendon of the long head of the biceps is most commonly implicated with tendonitis. When this tendon is subjected to repetitive stresses, it can become irritated, swollen, and painful.This occurs where the tendon sits within the bicipital groove at the top of the humerus under the transverse ligament before it becomes part of the shoulder joint capsule.