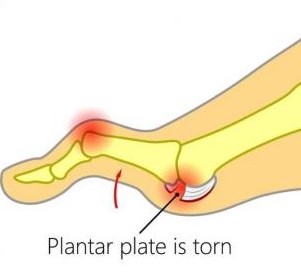
Plantar plate injuries are easily missed, probably because a lot of people don’t know what the plantar plate is. Quite they are diagnosed under the general term metatarsalgia. The plantar plate is a deep fibrocartilaginous structure that originates from the metatarsal head and attaches to the proximal phalanx through the joint capsule within the forefoot. Its role is to help stabilize the metatarsophalangeal joints (MTPJ), along with a couple of other structures. The plantar plate also acts as an attachment site for the plantar fascia, so if you load the foot, the medial arch lengthens, the plantar fascia tightens, this engages the plantar plate to plantarflex the proximal phalanx until the toe reaches the ground. This is a simplification of a complex process and is commonly known as the The ‘reversed’ windlass mechanism (with weight-bearing the longitudinal arch flattens, the foot lengthens, the plantar fascia tightens, the proximal phalanx becomes plantarflexed and the mechanism comes to a stop when the proximal phalanx presses against the ground).
What causes a plantar plate injury and how common are they?
There are many contributing factors. The first is any activity that exposes the MTPJ to repetitive and excessive dorsiflexion, so think about jumping and running especially in forefoot runners. There are a few biomechanical conditions that increase the load through the plantar plate such as hallux valgus (bunions). As the function through the 1st MTPJ(big toe) is reduced, then we get what is known as low gear propulsion and increased loading through lesser MTPJs, typically the 2nd, 1st, then 3rd and so on. Another condition like having say an irregular metatarsal length, for example, if you have a long 3rd metatarsal, can expose the plantar plate to increased load, as can external factors like high heels. Basically anything that will result in excessive dorsiflexion or ground reaction forces at the MTPJs may increase plantar plate loading.
How does a plantar plate injury present?..
The patient will complain of pain on the dorsal and plantar aspects of the MTPJ, usually described as an ache or bruising.
Mild oedema may be present along with an episode of trauma, however, trauma is not essential as plantar plate injuries are typically a chronic overuse injury
Reduced plantarflexion strength – The ‘Digital Purchase’ test
A quick way to do this, put a piece of paper under the apex of the affected toe and ask the patient to try and stop you pulling the paper away, in a plantar plate injury you will notice the paper is pulled away much more easily.
Pain, oedema and positive Digital Lachmans (Anterior Draw) / Vertical Stress.
Floating toe, if late-stage hammertoe, or Churchill sign may be present.
Diagnosis of plantar plate injuries
Digital Lachmans / Vertical Stress Test (Fig 1)
Same style of test to assess ACL tears, helps to assess the integrity of the plantar plate, it is quick, easy and a simple test to perform. Stabilise the head of the metatarsal with one hand, using the other hand stabilise the base of the proximal phalanx, apply a vertical force, we are looking for pain and any translocation, it is important to remember this is different from dorsiflexion of the digit.
Fig. 1
There are 2 scoring systems one by Thompson and Hamilton and the other Yu and Judge
Thompson and Hamilton
Stage 0, there is no dorsal translocation present of the proximal phalanx.
Stage 1 the base of the phalanx, will not dislocate, however, may sublux
Stage 2 the base of the phalanx can be dislocated.
Stage 3 the phalanx base is in a fixed dislocated position
Yu and Judge
Stage 1 mild odema on the plantar MTPJ with dorsal odema often present as well. Tenderness is present on palpation, however no anatomical malalignment.
Stage 2 moderate odema is present with a noticeable deviation.
Stage 3 odema present around the entire MTPJ with deviation and possible dislocation/subluxation, the odema will reduce however the deformities will remain.
I think the best way to describe the 2 different methods of testing, would be that the Thompson and Hamilton test best describes the integrity of the plantar plate at any given time, whereas the Yu and Judge test describes different stages based on clinical findings on the time of examination.
MRIs, X-rays and Ultrasound
There is still some debate as to whether an MRI scan or ultrasound scan is best for detecting plantar plate injuries. As we know ultrasound is cheaper, however, it is user-dependent, whereas MRI scan is more expensive but we can also get an overall picture of the structures within that area as well. X-ray in weight-bearing (lateral or oblique views) will show subluxation dorsally of the proximal phalanx on the metatarsal head, an anterior-posterior view will show a transverse deformity as well. An x-ray will also rule out other bony pathologies.12
Treatment of plantar plate injuries
The aim of treatments, like most musculoskeletal pathologies, is about managing the load. Essentially we want to try and reduce the ground reaction forces under the affected metatarsal head and reduce the plantarflexion moment of the metatarsal and the dorsiflexion of the phalanx.
Treatment protocols include
No barefoot walking/activity modification
Footwear advice / Air cast boot – we want to look at using a stiff-soled shoe, or reducing the heel height of a shoe, so footwear like high heels and the flexible minimalist type shoes tend to aggravate a plantar plate injury, the same goes for open-toe shoes and flip-flops, as you must claw your toes to keep these on which again increases the ground reaction force underneath the metatarsal.
Stretching / Strengthening – thinking about the mechanics of the foot, if there is tightness within the calf muscles, in turn, could result in early and increased loading through the forefoot, and if you are unable to get adequate dorsiflexion due to calf tightness, then the foot may pronate to compensate for this, which in turn could increase the loading through the lesser MTPJ’s. It is important also to work on strengthening the muscles within the foot.
Strapping can be very helpful in reducing pain, using a rigid zinc oxide tape and pulling the toe into a plantarflexed position to help offload a plantar plate (Fig 2).
Fig. 2 Strapping for plantar plate injury
Orthotics
Orthotics can be a useful way to help offload the affected plantar plate. One of the best ways to treat Plantar Plate Injures with or without surgery is using an orthotic device that places the pressure into the archway and off of the ball of the foot. If manufactured and molded correctly, they can keep the tension off the injury and pressure when standing and walking. Combining the orthoses with taping and footwear advice can be quite an effective way of offloading the affected plantar plate, whilst the patient reduces sporting activities.
Steroid injections
Steroid injections can be tried , however repeated intra-articular injections has been shown to result in dislocation of the MTPJ. It has also been suggested that injections into a ligament resulted in destruction of fibrocytes and reduction in tensile strength for up to 1 year which in turn may result in further damage a possible rupture.
A recent case study showing a patient with a plantar plate tear was managed using conservative measures, consisting of taping, activity modification and the use of a Darco boot over a 6 month period, and progressing to stiffed shoe and orthoses and stopped taping. At the 1 year mark, the patient was pain-free with no toe deformity, and on MRI the plantar plate has healed.
So what’s my treatment plan?
No barefoot walking for 6 weeks (minimum)
To wear stiff-soled shoes
Strapping of digit changing every 72 hours
Activity modification
Orthoses as described as above, plus any other modifications required
Stretching and Strength work – Distal and proximal
If conservative measures fail, then it may require referral to a surgeon.
Physiotherapist in Tralee. Ring to discuss your condition, to get a second opinion or to make an appointment. Click here for website.
Peroneal tendonitis occurs when the peroneal tendons become inflamed. This happens when there is an increased load on and/or overuse of the tendons. This causes the tendons to thicken over time. If the injury becomes chronic, the tendinitis can progress to tendinosis. This is more serious and takes longer to treat.
Peroneal tendonitis is particularly common in athletes especially runners , more so if their feet roll outwards during gait(over supination).
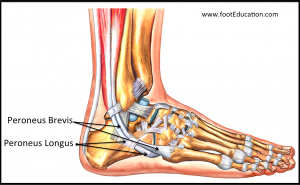
There are two peroneal tendons in each leg peroneus brevis and peroneus longus. They run side by side down the outside of the lower leg bone (fibula) and behind the bony lump on the outside of the ankle, the lateral malleolus. One peroneal tendon attaches to the outside of the foot at the base of the little toe (fifth metatarsal). The other tendon goes underneath the foot and attaches to the inside of the arch.The peroneal tendons provide stability to the ankle when it is bearing weight and protects it from sprains. They also help turn the foot out and stabilize the arch when walking.
Causes of Peroneal tendonitis
People who take part in a sport that involves repetitive ankle motion are most prone to peroneal tendonitis Factors that can contribute to peroneal tendonitis include:
overuse
a sudden increase in training, particularly weight-bearing activities, such as walking, running, and jumping
improper training techniques
inadequate or un-supportive footwear
There are also some other issues that can increase a person’s risk of developing peroneal tendonitis:
higher foot arches
lower limb muscles and joints not working well together
imbalanced muscles in the lower limbs
If someone fails to complete a rehabilitation program following an ankle injury, such as a sprain, they are also more likely to develop peroneal tendonitis. Over time, the damaged peroneal tendons will thicken as scar tissue tries to repair the damaged area. This makes the tendons weaker and more prone to tearing. Treatment can include orthotics to support the foot and take pressure off the tendon, wearing well laced up supportive footwear, very specific rehab program. Also instrument assisted soft tissue work seems to be beneficial, stripping out the tendon and promoting healing.
Bunions develop slowly. The big toe is made up of two joints. A bunion is a painful bony bump, also known as hallux valgus that develops on the inside of the foot at the big toe joint. Pressure on the big toe joint causes it to bend inwards towards the second toe. Over time, the normal structure of the joint changes, resulting in a bunion. The enlarged joint is often inflamed. The deformity gradually increases making it painful to wear shoes or walk. Bunions are more common in women. Many women wear tight, narrow shoes that squeeze the toes together. This makes it more likely for a bunion to develop. In most cases, bunion pain is relieved by wearing wider shoes with adequate toe room and using other simple treatments to reduce pressure on the big toe.
Bunion Progression
An advanced bunion can greatly alter the appearance of the foot. In severe bunions, the big toe may angle all the way under or over the second toe. Pressure from the big toe may force the second toe out of alignment, causing it to come in contact with the third toe. Calluses may develop where the toes rub against each other, causing additional discomfort and difficulty walking.
Foot Problems Related to Bunions
In some cases, an enlarged big toe joint may lead to bursitis, a painful condition in which the fluid-filled sac (bursa) that cushions the bone near the joint becomes inflamed. It may also lead to chronic pain and arthritis if the smooth articular cartilage that covers the joint becomes damaged from the joint not gliding smoothly.
Causes
Bunions may be caused by:
Wearing poorly fitting shoes—in particular, shoes with a narrow, pointed toe box that forces the toes into an unnatural position
Heredity—some people inherit feet that are more likely to develop bunions due to their shape and structure
Having an inflammatory condition, such as rheumatoid arthritis, or a neuromuscular condition, such as polio.
Diagnosis of bunions
Physical examination of bunions
Your doctor will ask you about your medical history, general health, and symptoms. He or she will perform a careful examination of your foot. Although your doctor will probably be able to diagnose your bunion based on your symptoms and on the appearance of your toe, he or she will also order an x-ray.
X-Rays
X-rays provide images of dense structures, such as bone. An x-ray will allow your doctor to check the alignment of your toes and look for damage to the MTP joint.
Nonsurgical treatment of bunions
In most cases, bunions are treated without surgery. Although nonsurgical treatment cannot actually “reverse” a bunion, it can help reduce pain and keep the bunion from worsening.
Changes in Footwear
In the vast majority of cases, bunion pain can be managed successfully by switching to shoes that fit properly and do not compress the toes.
Padding
Protective “bunion-shield” pads can help cushion the painful area over the bunion. Pads can be purchased at a drugstore or pharmacy. Be sure to test the pads for a short time period first; the size of the pad may increase the pressure on the bump. This could worsen your pain rather than reduce it.
Orthotics and Other Devices
Orthotics (custom-made shoe inserts) may be used to take pressure off your bunion. Toe spacers can also be placed between your toes to try and straighten the big toe. In some cases, a splint worn at night that places your big toe in a straighter position may help relieve pain.
Icing
Applying ice several times a day for 20 minutes at a time can help reduce swelling. Do not apply ice directly on your skin.
Medications
Nonsteroidal anti-inflammatory medications such as ibuprofen can help relieve pain and reduce swelling. Other medications can be prescribed to help pain and swelling in patients whose bunions are caused by arthritis.
Bunions and surgery
Your doctor may recommend surgery for a bunion, after a period of time, if you still have pain and difficulty walking despite changes in footwear and other nonsurgical treatments. Bunion surgery realigns bone, ligaments, tendons, and nerves so that the big toe can be brought back to its correct position.
Physiotherapists in Tralee stocking a wide range of orthotics to treat various foot conditions. Phone 0867700191
Equinus Foot Condition
The ankle joint connects the leg to the foot. It is formed by three separate bones, the tibia, fibula and talus. The shinbone (tibia) supports most of a person’s weight when standing. The outer bone (fibula) is the smaller bone of the lower leg. A small, irregular-shaped foot bone (talus) connects the tibia and fibula. Acting as a hinge, these bones form the ankle. The ankle joint allows movement such as walking, running and jumping, and also contributes to lower limb stability.
The ankle is reinforced by ligaments which connect bone to bone. Ligaments have a mildly elastic structure that allows them to stretch, within their limits, and then return to their normal positions. Ligaments protect the ankle from abnormal movements—especially twisting, turning and rolling of the foot.
Description
A person with equinus has a limited range of ankle motion and lacks the flexibility needed to bring the top of the foot upward, toward the shin. It may be either congenital or acquired, and occurs equally in both men and women. Equinus can be due to several different reasons including the following:
• bony block between the talus and distal tibia (osseous equinus);
• contracture or tightness of the soleus muscle (inner calf muscle);
• contracture or tightness of the soleus and gastrocnemius muscles (gastroc-soleal equinus);
• isolated tightness of the gastrocnemius muscles (outer calf muscle); and
• compensatory loss of ankle joint range of motion for some other condition such as pes cavus (pseudoequinus).
People with equinus often develop ways to compensate for their limited ankle motion. Depending on how a patient compensates for the inability to bend properly at the ankle, a variety of other foot conditions can develop, such as:
Plantar Fasciitis
Calf cramping
Achilles Tendinitis
Metatarsalgia (pain and/or callusing on the ball of the foot)
Flatfoot
Arthritis of the midfoot (middle area of the foot)
Pressure sores on the ball of the foot or the arch
Bunions and hammertoes
Ankle pain
Shin splints
Sesamoiditis
Hallux valgus
hallux rigidus
Hammer toes
Nonsurgical Treatment of Equinus
Some nonsurgical treatment strategies are aimed at relieving the symptoms and conditions associated with equinus. Treatment for the equinus itself may include one or more of the following options.
Heel lifts—Placing heel lifts inside the shoes or wearing shoes with a moderate heel may reduce symptoms by taking stress off the Achilles tendon and compensating for the restricted movement of the ankle joint. The joint is meant to have about fourteen degrees of movement ideally, so say it has only four degrees of movement, adding a ten degree heel lift helps compensate for the missing degrees of movement .
Arch supports or orthotic devices—Custom orthotic devices that fit into the shoe are often prescribed to ensure that weight is distributed properly, and to help control muscle/tendon imbalance. Again these devices will most likely include a heel lift.
Physical therapy—To help remedy muscle tightness, deep tissue massage of calf muscles along with a stretching program for the calf muscles are recommended.
For a quick simple video describing the condition click here
Big toe joint arthritis (otherwise known as Hallux Rigidus) is a form of degenerative arthritis. In this condition, surfaces of the joints in the big toe begin to wear away and extra bone can also develop in the form of bone spurs or osteophytes. This limits the movement of the joint. The big toe needs to bend significantly when stepping off. Consequently, arthritis in this joint can greatly affect walking, running etc.
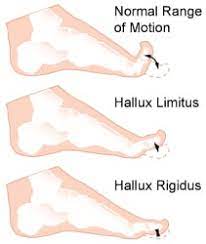
Hallux Rigidus is a condition that tends to get worse over time. In it’s earlier stages, it may be referred to as Hallux Limitus, which is where there is limited movement of the big toe joint. With progression, Hallux Rigidus develops which can result in stiffness developing in the big toe joint and there may also be swelling.
To compensate for pain in the big toe joint, people with Hallux Rigidus tend to adjust their walking pattern which can also result in knee, hip or lower back pain. There is often difficulty finding shoes that fit properly shoes due to pain and/or inflammation in the joint. Early diagnosis can be made by physical examination and x-ray. Early treatment gives the best chance of avoiding surgery.
What causes Hallux Rigidus?
The big toe joint is designed to bear a considerable amount of stress during walking. However faulty biomechanics or structural abnormalities such as flat feet can stop the big toe from bending normally, and eventually lead to the development of osteoarthritis in the big toe joint. Other factors that can increase the risk of developing this condition include genetics (eg, having a certain foot type), injury to the big toe , other inflammatory diseases, and working in a job that places excessive stress on the big toe joint .
Treatment
In cases of Hallux Rigidus, certain types of footwear and orthotics may be recommended to reduce pressure and motion on the big toe. Custom orthotics that conform very closely to the arch of the foot are most effective in improving big toe joint function. These orthotics may incorporate something like a 3mm kinetic wedge in combination with a built in forefoot posting to take the pressure off the big toe joint. Ice and anti-inflammatory medication can also be used to reduce inflammation and pain. If it does not respond to conservative treatment, surgery may be recommended as a last resort in more severe cases.
Metatarsalgia
Metatarsalgia is the name given to pain in the front part of your foot under the heads of your metatarsal bones ( ball of foot, just before toes). It is usually worse when standing or walking etc. and occurs most frequently in the second, third/or fourth metatarsal joints or isolated in the first metatarsal joint. Metatarsalgia usually comes on gradually over some weeks rather than suddenly. The affected area of your foot may also feel tender on palpation by your physiotherapist.
Causes
Common causes identified by physiotherapists include:
Pes cavus or high arched foot.
Excessive pronation of the foot(foot rools inwards ie. with flat foot).
Clawing or hammer toes.
Tight extensor tendons of the toes.
Prominent metatarsal heads.
Morton’s foot – here there is a shortened first metatarsal, which results in an abnormal gait putting increased pressure on the second metarsal.
Over doing it in athletes such as runners and tennis players etc. can lead to inflammation in the joints due to the pounding they receive.
Being overweight puts extra stress on many areas of the foot including metatarsals.
Wearing high heels – forward force on feet increases the pressure on metatarsal area.
Having tightened calf muscles or poor ankle flexibility – this affects the normal gait pattern.
Poorly fitting or tight footwear can squeeze the metatarsal joints causing friction , inflammation and poor gait.
Treatment
Simple measures can help to relieve the symptoms of metatarsalgia. These include:
Resting with your feet elevated where possible.
Losing weight if you are overweight.
Wearing supportive shoes that are well fitted, low-heeled and have a wide toe area.
Metatarsal pads and orthotic inserts for your shoes may help to relieve pain in your forefoot by reducing the pressure placed on the heads of your metatarsal bones.
Physiotherapy may also be helpful. This may include stretching out the spaces between the metatarsal and mobilising the joints of the foot or performing deep tissue massage to loosen your calf muscles or any other lower limb muscles that may be contributing to poor gait. Sometimes if a metatarsal head has dropped it can be manipulated back into place. Pain relief as a result of this mobilisation, when effective can be immense and long lasting.
Simple painkillers such as paracetamol and non-steroidal anti-inflammatories(NSAIDs) such as ibuprofen may help to relieve pain.
Plantar Fasciitis – Foot Pain
Plantar fasciitis is a painful inflammatory condition of the connective tissue on the sole of the foot(the plantar fascia). It is often caused by overuse of the plantar fascia, the tendons that help form the arch of the foot , running from the heel along the sole of the foot towards the toes. The plantar fasciabasically acts as shock absorber for the foot during movement while helping maintain the arch of the foot during standing. Plantar fasciitis is easiest treated when caught early. Longstanding cases often demonstrate more degenerative changes in the tissue than just inflammatory changes. This condition is called termedplantar fasciosis and can be much more difficult to treat.
While plantar fasciitis is often attributed to overuse inathletes, among non-athletic populations it is associated with a high body mass index in combination withlong periods of weight bearing( Mc Poil et al. 2008).Also people with flat feet or high arches tend to be more at risk. A Flat foot tends to put increased strain on the origin of the plantar fascia at the heel (calcaneus) as the plantar fascia attempts to maintain a stable arch during the propulsive stage of the gait(walking, running etc.). Excessive movement of the forefoot in relation to the heelduring movement can also predispose to plantar fasciitis. In people with high arches there may be excessive strain on the heel due to the foots limited range of movement and thus a decreased ability to adaptto the ground during movement.
Plantar fasciitis is commonly also associated with tightness in the calves, hamstrings and gluteal regions. Muscles in these areas have a significant effect on gait and thus foot biomechanics . Biomechanics is basically the science of movement, so when you here the phrase ”poor biomechanics” used it is basically referring to inefficiency during movement.
With the condition the pain is usually gradual in onset and felt on the medial aspect of the heel. Initially it is worse in the morning and decreases with activity, often aching afterwards. Periods of inactivity during the day are generally followed by an increase in pain as activity is recommenced. As the condition becomes more severe, the pain may be present when weight-bearing and worsen with activity.
Treatment
Effective treatment uses a multifaceted approach which may involve some or all of the following ; the use of nonsteroidal anti-inflammatory drugs (NSAIDs), deep tissue massage of the plantar fascia and along with deep tissue work to loosen out the calves, hamstrings and gluteal regions where necessary, stretching exercises for the plantar fascia(DiGiovanniet al. 2003) and calf muscles, avoidance of aggravating activity, biomechanical correction with orthotics, electro-acupuncture and cold compression of the heel bursitis, strengthening exercises for the intrinsic muscles of the feet(Dyck and O’Neill ,2004), taping the heel into inversion (short term solution)( Radfordet al. 2006), changing to proper supportive footwear containing well supported arches and midsoles (Yamashita, M.H. 2005). In extreme cases when all else has failed corticosteroid injections may be considered if there is a bursitis in the heel (Crawford et al. 1999) with surgery used as a last resort. This condition is usually resolved swiftly by an experienced practitioner without the need for surgery or corticosteroid injections.
Physiotherapist based in Tralee , Co. Kerry and open 7am to 11 pm weekdays, 7am to 2pm Saturdays.Please ring 086-7700191 anytime to make an appointment. We also specialize in proper deep tissue massage.
References
Crawford, E., Atkins, D., Young, P. et al. Steroid injection for heel pain: evidence of short term effectiveness: a randomized controlled trial. Rheumatology 1999;38(10):974-7.
DiGiovanni, B.F., Nawoczenski, D.A., Lintal, M.E. et al. Tissue-specific plantar fascia-stretching exercise enhances outcomes in patients with chronic heel pain. A prospective randomized study. J. Bone Joint Surg. Am. 2003;85-A(7):1270-7.
McPoil, T.G., Martin, R.R.L., Cornwall, M.W. et al. Heel pain – plantar fasciitis: clinical practice guidelines linked to the international classification of functioning, disability, and health from the orthopedic section of the American Physical Therapy Association. J. Orthop. Sports Phys. Ther. 2008;38(4): A1-18.
Radford, J.A., Landorf, K.B., BuchbinderR. et al. Effectiveness of low-dye taping foe the short-term treatment of plantar heel: a randomised trial. B.M.C.
Yamashita, M.H. Evaluation and selection of shoe wear and orthoses for the runner. Phys. Med. Rehabil. Clin. N. Am. 2005;16:801-29.


 Peroneal tendonitis occurs when the peroneal tendons become inflamed. This happens when there is an increased load on and/or overuse of the tendons. This causes the tendons to thicken over time. If the injury becomes chronic, the tendinitis can progress to tendinosis. This is more serious and takes longer to treat.
Peroneal tendonitis occurs when the peroneal tendons become inflamed. This happens when there is an increased load on and/or overuse of the tendons. This causes the tendons to thicken over time. If the injury becomes chronic, the tendinitis can progress to tendinosis. This is more serious and takes longer to treat.
 Metatarsalgia is the name given to pain in the front part of your foot under the heads of your metatarsal bones ( ball of foot, just before toes). It is usually worse when standing or walking etc. and occurs most frequently in the second, third/or fourth metatarsal joints or isolated in the first metatarsal joint. Metatarsalgia usually comes on gradually over some weeks rather than suddenly. The affected area of your foot may also feel tender on palpation by your physiotherapist.
Metatarsalgia is the name given to pain in the front part of your foot under the heads of your metatarsal bones ( ball of foot, just before toes). It is usually worse when standing or walking etc. and occurs most frequently in the second, third/or fourth metatarsal joints or isolated in the first metatarsal joint. Metatarsalgia usually comes on gradually over some weeks rather than suddenly. The affected area of your foot may also feel tender on palpation by your physiotherapist. Plantar fasciitis is a painful inflammatory condition of the connective tissue on the sole of the foot(the plantar fascia). It is often caused by overuse of the plantar fascia, the tendons that help form the arch of the foot , running from the heel along the sole of the foot towards the toes. The plantar fascia
Plantar fasciitis is a painful inflammatory condition of the connective tissue on the sole of the foot(the plantar fascia). It is often caused by overuse of the plantar fascia, the tendons that help form the arch of the foot , running from the heel along the sole of the foot towards the toes. The plantar fascia