Tennis Elbow Misdiagnosis
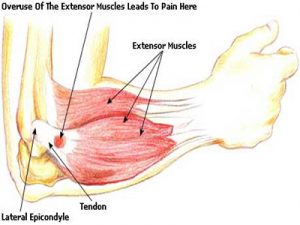
Tennis elbow, or lateral epicondylitis, is a painful condition of the elbow usually caused by overuse. Muscles, ligaments, and tendons support the functioning of the elbow joint. Your forearm extensor muscles and tendons extend the wrist and fingers. These extensor tendons attach the forearm muscles on the outside of the elbow to the lateral epicondyle. Tennis elbow is an injury to these tendons leading to pain and tenderness on the outside of the elbow. The main tendon involved in tennis elbow is usually the ”extensor carpi radialis brevis” tendon . Tennis elbow misdiagnosis is relatively common.
Tennis Elbow
When the tendon is weakened from overuse or trauma , microscopic tears form in the where the tendon attaches to the lateral epicondyle. This leads to pain and inflammation. The extensor carpi radialis brevis tendon may also be at increased risk of damage due to its position. As the elbow bends and straightens, the tendon rubs against the bone. This repetitive action can cause gradual wear and tear on the tendon over time in certain activities.
Activities – cause
Athletes are not the only people who get tennis elbow. Many people with tennis elbow participate in work or recreational activities that require repetitive and vigorous use of the forearm muscle. Painters, plumbers, carpenters, hairdressers, barbers, butchers(boners), people cutting hedges with clippers for long periods, are all particularly prone to developing tennis elbow.
Misdiagnosis
Tennis elbow misdiagnosis and mismanagement of this condition is often why people fail to recover. There are two common areas of misdiagnosis. Firstly if a person has not been doing any repetitive work with their forearm and there has been no forceful trauma while using the forearm, it is unlikely that the condition is tennis elbow. Sometimes the actual issue here is nerve pain radiating down the arm from nerve compression in the neck and/or shoulder(neuropraxia). This nerve compression can be due to tight muscles/ locked facet joints and/or misaligned structures, often due to poor posture. In the second type of tennis elbow misdiagnosis there can be repetitive injury involved but the condition is being exacerbated by nerve compression in the neck and shoulders, so both all areas need to be looked at for full resolution.
A cortisone injection is often used to try and treat ”tennis elbow”. This at most usually only gives short term relief and can even exacerbate the condition long-term with true tennis elbow, as it often allows the person to return to the aggravating activity thinking the injury has healed. Cortisone is an anti-inflammatory and may decrease inflammation in the area, reducing pain. It does not however stimulate tendon repair, which is what has been damaged in true ”tennis elbow” . Neither does cortisone do anything for a trapped nerve.
The above conditions are where an experienced physiotherapist/physical therapist can help greatly, usually much more so than any medication. This is their area of expertise. However, you always need to remember accurate diagnosis and effective treatment is very practitioner dependent. Eccentric training along with soft tissue work can be very effective for true ”tennis elbow”. For the nerve compression (neuropraxia) described above, soft tissue release of neck and shoulder muscles(levator scapulae, trapezius,scalenes etc.) along with osteopathic manipulations to release any locked cervical or thoracic facet joints can be very effective. Symptoms of nerve entrapment/involvement can include neck/shoulder pain with tingling down the arms and/or into fingers. There are also manual orthopedic tests to check for nerve entrapment.
Aside : Carpal Tunnel syndrome is a medical condition due to compression of the median nerve as it travels through the wrist at the carpal tunnel. This can also be misdiagnosed and be due to nerve compression in neck /shoulder or upper thoracic regions.
Physiotherapists in Tralee phone 086-7700191