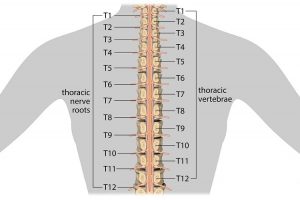
A mobile thoracic spine allows you turn your back in many directions, enabling you to do everyday tasks with ease. Today’s sedentary lifestyle often contributes to reduced spinal mobility. Basically ”motion is lotion” and if you are inactive and also prone to poor posture, your thoracic spine can seize up. If it goes on long enough, say into old age portions of the spine may fuse and not move at all. A lack of thoracic spine mobility means that the lumbar spine, pelvis, shoulders and surrounding muscles have to compensate. Long term, these over-compensations can lead to overuse conditions and injuries, the lower back being particularly suceptable. This is because the lumbar spine is meant to keep us stable and is not very mobile, so when these joints are forced to overcompensate for the lack of movement in the thoracic area, it can place alot of pressure on the discs of the lower back. Possible consequences include inflammation, degeneration, herniation of the discs, generalized low back pain, compression fractures, muscles spasms, and spinal nerve injuries. Similar pressures and injuries can occur in the neck and shoulders. For example, if your thoracic spine isn’t mobile, anytime you have to do a movement overhead, your shoulders make up for that lack of mobility. If you have shoulder impingement or chronic shoulder and neck problems lack of mobility in the thoracic spine will make every thing worse.
Improving Thoracic Spine Mobility
Yoga, pre- and post-workout stretching, and mobility exercises are the best way of maintaining and improving thoracic spine mobility. These need to be done regularly and consistently, especially as you get older. Your physiotherapist will be able to guide you on the correct exercises and help correct your form and technique until you get used to them and can do them yourself. Here are a few exercises to get you started.
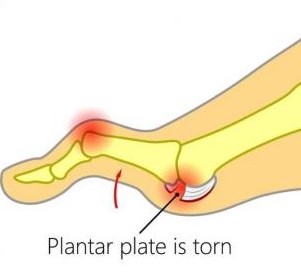
Plantar plate injuries are easily missed, probably because a lot of people don’t know what the plantar plate is. Quite they are diagnosed under the general term metatarsalgia. The plantar plate is a deep fibrocartilaginous structure that originates from the metatarsal head and attaches to the proximal phalanx through the joint capsule within the forefoot. Its role is to help stabilize the metatarsophalangeal joints (MTPJ), along with a couple of other structures. The plantar plate also acts as an attachment site for the plantar fascia, so if you load the foot, the medial arch lengthens, the plantar fascia tightens, this engages the plantar plate to plantarflex the proximal phalanx until the toe reaches the ground. This is a simplification of a complex process and is commonly known as the The ‘reversed’ windlass mechanism (with weight-bearing the longitudinal arch flattens, the foot lengthens, the plantar fascia tightens, the proximal phalanx becomes plantarflexed and the mechanism comes to a stop when the proximal phalanx presses against the ground).
What causes a plantar plate injury and how common are they?
There are many contributing factors. The first is any activity that exposes the MTPJ to repetitive and excessive dorsiflexion, so think about jumping and running especially in forefoot runners. There are a few biomechanical conditions that increase the load through the plantar plate such as hallux valgus (bunions). As the function through the 1st MTPJ(big toe) is reduced, then we get what is known as low gear propulsion and increased loading through lesser MTPJs, typically the 2nd, 1st, then 3rd and so on. Another condition like having say an irregular metatarsal length, for example, if you have a long 3rd metatarsal, can expose the plantar plate to increased load, as can external factors like high heels. Basically anything that will result in excessive dorsiflexion or ground reaction forces at the MTPJs may increase plantar plate loading.
How does a plantar plate injury present?..
The patient will complain of pain on the dorsal and plantar aspects of the MTPJ, usually described as an ache or bruising.
Mild oedema may be present along with an episode of trauma, however, trauma is not essential as plantar plate injuries are typically a chronic overuse injury
Reduced plantarflexion strength – The ‘Digital Purchase’ test
A quick way to do this, put a piece of paper under the apex of the affected toe and ask the patient to try and stop you pulling the paper away, in a plantar plate injury you will notice the paper is pulled away much more easily.
Pain, oedema and positive Digital Lachmans (Anterior Draw) / Vertical Stress.
Floating toe, if late-stage hammertoe, or Churchill sign may be present.
Diagnosis of plantar plate injuries
Digital Lachmans / Vertical Stress Test (Fig 1)
Same style of test to assess ACL tears, helps to assess the integrity of the plantar plate, it is quick, easy and a simple test to perform. Stabilise the head of the metatarsal with one hand, using the other hand stabilise the base of the proximal phalanx, apply a vertical force, we are looking for pain and any translocation, it is important to remember this is different from dorsiflexion of the digit.
Fig. 1
There are 2 scoring systems one by Thompson and Hamilton and the other Yu and Judge
Thompson and Hamilton
Stage 0, there is no dorsal translocation present of the proximal phalanx.
Stage 1 the base of the phalanx, will not dislocate, however, may sublux
Stage 2 the base of the phalanx can be dislocated.
Stage 3 the phalanx base is in a fixed dislocated position
Yu and Judge
Stage 1 mild odema on the plantar MTPJ with dorsal odema often present as well. Tenderness is present on palpation, however no anatomical malalignment.
Stage 2 moderate odema is present with a noticeable deviation.
Stage 3 odema present around the entire MTPJ with deviation and possible dislocation/subluxation, the odema will reduce however the deformities will remain.
I think the best way to describe the 2 different methods of testing, would be that the Thompson and Hamilton test best describes the integrity of the plantar plate at any given time, whereas the Yu and Judge test describes different stages based on clinical findings on the time of examination.
MRIs, X-rays and Ultrasound
There is still some debate as to whether an MRI scan or ultrasound scan is best for detecting plantar plate injuries. As we know ultrasound is cheaper, however, it is user-dependent, whereas MRI scan is more expensive but we can also get an overall picture of the structures within that area as well. X-ray in weight-bearing (lateral or oblique views) will show subluxation dorsally of the proximal phalanx on the metatarsal head, an anterior-posterior view will show a transverse deformity as well. An x-ray will also rule out other bony pathologies.12
Treatment of plantar plate injuries
The aim of treatments, like most musculoskeletal pathologies, is about managing the load. Essentially we want to try and reduce the ground reaction forces under the affected metatarsal head and reduce the plantarflexion moment of the metatarsal and the dorsiflexion of the phalanx.
Treatment protocols include
No barefoot walking/activity modification
Footwear advice / Air cast boot – we want to look at using a stiff-soled shoe, or reducing the heel height of a shoe, so footwear like high heels and the flexible minimalist type shoes tend to aggravate a plantar plate injury, the same goes for open-toe shoes and flip-flops, as you must claw your toes to keep these on which again increases the ground reaction force underneath the metatarsal.
Stretching / Strengthening – thinking about the mechanics of the foot, if there is tightness within the calf muscles, in turn, could result in early and increased loading through the forefoot, and if you are unable to get adequate dorsiflexion due to calf tightness, then the foot may pronate to compensate for this, which in turn could increase the loading through the lesser MTPJ’s. It is important also to work on strengthening the muscles within the foot.
Strapping can be very helpful in reducing pain, using a rigid zinc oxide tape and pulling the toe into a plantarflexed position to help offload a plantar plate (Fig 2).
Fig. 2 Strapping for plantar plate injury
Orthotics
Orthotics can be a useful way to help offload the affected plantar plate. One of the best ways to treat Plantar Plate Injures with or without surgery is using an orthotic device that places the pressure into the archway and off of the ball of the foot. If manufactured and molded correctly, they can keep the tension off the injury and pressure when standing and walking. Combining the orthoses with taping and footwear advice can be quite an effective way of offloading the affected plantar plate, whilst the patient reduces sporting activities.
Steroid injections
Steroid injections can be tried , however repeated intra-articular injections has been shown to result in dislocation of the MTPJ. It has also been suggested that injections into a ligament resulted in destruction of fibrocytes and reduction in tensile strength for up to 1 year which in turn may result in further damage a possible rupture.
A recent case study showing a patient with a plantar plate tear was managed using conservative measures, consisting of taping, activity modification and the use of a Darco boot over a 6 month period, and progressing to stiffed shoe and orthoses and stopped taping. At the 1 year mark, the patient was pain-free with no toe deformity, and on MRI the plantar plate has healed.
So what’s my treatment plan?
No barefoot walking for 6 weeks (minimum)
To wear stiff-soled shoes
Strapping of digit changing every 72 hours
Activity modification
Orthoses as described as above, plus any other modifications required
Stretching and Strength work – Distal and proximal
If conservative measures fail, then it may require referral to a surgeon.
Physiotherapist in Tralee. Ring to discuss your condition, to get a second opinion or to make an appointment. Click here for website.
Herniated Disc vs Bulging Disc
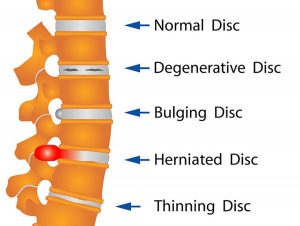
Your spine is made up of lots of bones called vertebrae and discs stacked on top of one another, forming the spinal canal. The nerves of the spinal cord run down the length of the spinal canal. The discs in act like shock absorbers between the vertebrae. These discs are made of two components: a softer center (called nucleus pulposus) surrounded by a tough elastic-like band (called annulus fibrosus). A bulging disc is like a squashed jam doughnut before the jam bursts out. The disc sags and looks like it is bulging outward. With a herniated disc, the outer covering of the disc has a hole or tear. This causes the nucleus pulposus (jelly-like center of the disc) to leak into the spinal canal. It is like the jam leaking out from the inside of a squashed jam doughnut.
Bulging discs are usually caused by age-related degeneration. There is usually a progressive, gradual onset of symptoms. Bulging discs and herniated discs can occur anywhere along the spine. Pain from a herniated disc usually comes on abruptly often affecting one individual nerve root. Herniated discs are often caused by an acute injury. In some cases, you may know the cause of the injury, such as twisting incorrectly.
Herniated and bulging discs are the most common causes of lower back pain, as well as leg pain or ”sciatica.” Between 60% and 80% of people will experience low back pain at some point their lives. Although a herniated disk can be very painful, most people feel much better with just a few weeks or months of nonsurgical treatment, such as using muscle relaxants and anti-inflammatory medications, along with physiotherapy. Long term management of these conditions needs to including properly prescribed strengthening and flexibility exercises in order to avoid surgery. Surgery is the final option.
For more on herniated and bulging discs, see video.
Physio in Tralee. Phone 0867700191 to discuss your condition or make an appointment.
Peroneal tendonitis occurs when the peroneal tendons become inflamed. This happens when there is an increased load on and/or overuse of the tendons. This causes the tendons to thicken over time. If the injury becomes chronic, the tendinitis can progress to tendinosis. This is more serious and takes longer to treat.
Peroneal tendonitis is particularly common in athletes especially runners , more so if their feet roll outwards during gait(over supination).
There are two peroneal tendons in each leg peroneus brevis and peroneus longus. They run side by side down the outside of the lower leg bone (fibula) and behind the bony lump on the outside of the ankle, the lateral malleolus. One peroneal tendon attaches to the outside of the foot at the base of the little toe (fifth metatarsal). The other tendon goes underneath the foot and attaches to the inside of the arch.The peroneal tendons provide stability to the ankle when it is bearing weight and protects it from sprains. They also help turn the foot out and stabilize the arch when walking.
Causes of Peroneal tendonitis
People who take part in a sport that involves repetitive ankle motion are most prone to peroneal tendonitis Factors that can contribute to peroneal tendonitis include:
overuse
a sudden increase in training, particularly weight-bearing activities, such as walking, running, and jumping
improper training techniques
inadequate or un-supportive footwear
There are also some other issues that can increase a person’s risk of developing peroneal tendonitis:
higher foot arches
lower limb muscles and joints not working well together
imbalanced muscles in the lower limbs
If someone fails to complete a rehabilitation program following an ankle injury, such as a sprain, they are also more likely to develop peroneal tendonitis. Over time, the damaged peroneal tendons will thicken as scar tissue tries to repair the damaged area. This makes the tendons weaker and more prone to tearing. Treatment can include orthotics to support the foot and take pressure off the tendon, wearing well laced up supportive footwear, very specific rehab program. Also instrument assisted soft tissue work seems to be beneficial, stripping out the tendon and promoting healing.
Meniscus injuries are a relatively common knee injury. Cartilage within the knee joint provides cushioning between the bones at this joint. This protects them from the stresses of walking, jumping, running etc. There is articular cartilage which is the smooth, white tissue that covers the ends of bones(Femur, tibia) where they come together to form the knee joint. Healthy cartilage in our joints makes it easier to move. It allows the bones to glide over each other with very little friction. Articular cartilage can be damaged by injury or normal wear and tear.
Within the knee you also have fibrocartilage in the form of the medial and lateral meniscii. These are two thick wedge-shaped pads of cartilage attached to top of the tibia (tibial plateau) and under the femur bone. They allow the femur to glide when the knee joint moves. Each meniscus is curved in a C-shape, with the front part of the cartilage called the anterior horn and the back part called the posterior horn. Meniscal tears are usually described by where they are located anatomically in the C shape and by their appearance (for example, “bucket handle” tear, longitudinal, parrot beak, and transverse).
Blood supply
Because the blood supply is different to each part of the meniscus. Knowing where the tear is located may help decide how easily an injury might heal (with or without surgery). The better the blood supply, the better the potential for recovery. The outside rim of cartilage has better blood supply than the central part of the “C.” Blood supply to knee cartilage also decreases with age, with up to 20% of normal blood supply lost by age 40.
What causes a meniscus to tear?
A forceful twist or sudden stop can cause the end of the femur to grind into the top of the tibia, pinching and potentially tearing the cartilage of the meniscus. These meniscus injuries can also occur with deep squatting or kneeling, especially when lifting a heavy weight. Meniscus tear injuries often occur during athletic activities, especially in contact sports like football and hockey. Motions that require pivoting and sudden stops, in sports like tennis, basketball, and golf, can also cause meniscus damage.
Meniscus injuries – Increasing risk with age
The risk of developing a torn meniscus increases with age. This is because cartilage begins to gradually wear out, losing its blood supply and its resilience. Being overweight also puts more stress on the meniscii. This means that routine daily activities like walking and climbing stairs increase the potential for wear, degeneration, and tearing. It is estimated that six out of 10 patients older than 65 years have a degenerative meniscus tear. Many of these tears may never cause problems.
Some of the fibers of the cartilage are interconnected with those of the ligaments that surround the knee. Thus, meniscus injuries may also be associated with tears of the collateral and cruciate ligaments, depending upon the mechanism of injury.
Symptoms of meniscus injuries can include some or all of the following:
Pain with running or walking longer distances
Intermittent swelling of the knee joint: Many times, the knee with a torn meniscus feels “tight.”
Popping, especially when climbing up or down stairs
Giving way or buckling (the sensation that the knee is unstable and the feeling that the knee will give way): Less commonly, the knee actually will give way and cause the patient to fall.
Locking (a mechanical block where the knee cannot be fully extended or straightened): This occurs when a piece of torn meniscus folds on itself and blocks full range of motion of the knee joint. The knee gets “stuck,” usually flexed between 15 and 30 degrees and cannot bend or straighten from that position.
Diagnosis
The diagnosis of a knee injury begins with a history of the injury etc. and physical examination. There have been many tests described to assess the internal structures of the knee. The McMurray test is one long used orthopedic test . The health-care professional flexes the knee and rotates the tibia while feeling along the joint. The test is positive for a potential tear if a click is felt or noticeable pain is felt while circumducting the knee in full flexion.
Physiotherapy in Tralee – referral for MRI
(MRI) is the test of choice to confirm the diagnosis of a torn meniscus. It also allows a radiographer to visualize the inner structures of the knee. These structure include; the cartilage and ligaments, the surface of the bones, and the muscles and tendons that surround the knee joint. Plain X-rays cannot be used to identify meniscal tears but may be helpful in looking for bony changes, including fractures, arthritis, and loose bony fragments within the joint. In older patients, X-rays may be taken of both knees while the patient is standing. This allows the joint spaces to be compared to assess the degree of cartilage wear. Cartilage takes up space within the joint and if the joint space is narrowed, it may be an indicator that there is less cartilage present, likely from degenerative disease.
Treatment of Meniscal Tears
Sometimes conservative measures such as physical therapy, NSAIDs and rest can be enough to settle the condition. When conservative measures are ineffective the next step may be surgery to repair or remove the damaged cartilage.
For physiotherapy in Tralee phone 086-7700191, click here for website homepage
Dry Needling
Trigger-point dry needling is a procedure where a fine acupuncture needle is inserted into the skin and muscle. It is aimed at myofascial trigger points, which are points of exquisite pain in skeletal muscle, that are associated with a hypersensitive palpable nodule or a taut band.
Active trigger points can spontaneously trigger local or referred pain. They cause muscle weakness, restricted range of movement and autonomic phenomena. Latent trigger points do not cause pain unless they are stimulated. They may alter muscle activation patterns and contribute to restricted range of movement . Therefore both active and latent trigger points cause allodynia(nerve pain) at the trigger point site and hyperalgesia away from the trigger point following applied pressure.
The formation of trigger points is caused by the creation of a taut band or knot within the muscle. This band is caused by excessive acetylcholine release from the motor endplate combined with inhibition of acetylcholine esterase and upregulation of nicotinic acetylcholine receptors. Motor end plates, also called neuromuscular junctions, are specialised chemical synapses formed at the sites where the terminal branches of the axon of a motor neuron contact a target muscle cell. Motor neurons are nerve cells that send electrical output signals to the muscles.
Initially the taut bands are produced as a normal protective, physiological measure in the presence of actual or potential muscle damage. They are thought to occur in response to unaccustomed eccentric or concentric loading, sustained postures and repetitive low load stress. However when sustained they contribute to sustained pain. The pain caused by trigger points is due to hypoxia and decreased blood flow within the trigger point. This leads to a decreased pH which activates the muscle nociceptors to restore homeostasis. This causes peripheral sensitization. Trigger points are also involved in central sensitization. The mechanism remains unclear but trigger points maintain nocioceptive input into the dorsal horn and therefore contribute to central sensitization.
Stimulation of a local twitch response (LTR)
Dry-needling of these myofascial trigger points via mechanical stimulation causes an analgesic effect. This mechanical stimulation causes a local twitch response (LTR). A LTR is an involuntary spinal cord reflex contraction of the muscle fibers in a taut band. Triggering an LTR has been shown to reduce the concentration of nociceptive substances in the chemical environment near myofascial trigger points.
Muscle regeneration
The needle may also cause a small focal lesion which triggers satellite cell migration to the area which then repair or replace damaged myofibers. This occurs 7-10 days after dry needling. It is unclear whether continued dry needling within this period may disrupt this process.
Dry needling may also cause a localized stretch to the cytoskeletal structures. This stretch may allow sarcomeres to resume their resting length. The mechanical pressure causes collagen fibers to intrinsically electrically polarize which also triggers tissue remodeling.
The effectiveness of this treatment depends greatly on the skill of the therapist to accurately palpate mysofascial trigger points.
Physiotherapists in Tralee specializing in hand-on deep tissue work, dry needling and osteopathic manipulations. Phone 0867700191 to discuss your condition or make an appointment.
Osgood Schlatterdisease : Knee Pain in Adolescents
Osgood Schlatter disease is an inflammation of the bone, cartilage and/or tendon at the top of the tibia (shinbone ie. just under the knee), where the tendon from the kneecap(patella) attaches. It presents as a painful lump below the kneecap. It usually strikes active adolescents during growth spurts which can begin any time between the ages of 8 and 13 in girls, 10 and 15 years in boys, basically during puberty. Growth spurts make kids vulnerable because their bones, muscles, and tendons are growing quickly and not always at the same time. With exercise, these differences in size and strength between the muscle groups place unusual stress on the growth plate at the top of the shinbone (A growth plate is a layer of cartilage near the end of a bone where most of the bone’s growth occurs. It is weaker and more vulnerable to injury than the rest of the bone).
While Osgood Schlatterdisease is more common in boys, the gender gap is narrowing as more girls become involved in sports. Osgood Schlatterdisease affects as many as 1 in 5 adolescent athletes. Teens increase their risk if they play sports involving running, twisting, and jumping, such as basketball, football, volleyball, soccer, tennis, figure skating, and gymnastics etc. Doctors disagree about the mechanics that cause the injury but agree that both overuse and physical stress are involved. Most parents call the doctor after their child complains of intermittent pain over several months.
Signs and symptoms of Osgood Schlatterdisease
pain that worsens with exercise
relief from pain with rest
swelling or tenderness at the bony prominence under the knee and over the shinbone
limping after exercise
tightness of the muscles surrounding the knee (the hamstring sometimes but particularly the quadriceps muscles)
The pain varies from person to person. Some have only mild pain while performing certain activities. For others, the pain is nearly constant and can be debilitating. The good news is that Osgood Schlatterdisease (OSD) is far less serious than its name suggests. Though it is one of the most common causes of knee pain in adolescents, it is really not a disease, but an overuse injury. The condition is self limiting and usually resolves itself within 12 to 24 months. A similar condition, ”Sever’s disease” occurs in children of the same age group down at the achilles tendon attachment and presents as heel pain. Again the condition is self limiting and the same treatment protocols apply.
While there is no evidence that rest accelerates the healing process, a reduction in activity usually reduces the pain. There is no need to rest completely. Pain should be the main guide as to limitation of activity. Tightness in the quadriceps muscles may predispose to this condition. The athlete should commence a stretching program. Some massage therapy on the quadriceps can be tried. Pain also can sometimes be relieved by icing the painful area(ice in wet towel) for 10 minutes at a time. Correction of any biomechanical abnormality, such as excessive subtalar pronation(feet turn out while running) should also be considered.
Summary
To sum up, this is basically a self limiting condition that adolescents generally grow out of (Brukner and Khan, 2011). Some stretching exercises and modification of activities is generally the best and most cost effective course of treatment.
Spinal stenosis is a narrowing of the spaces within your spine, which can put pressure on the nerves that travel through the spine. Others may experience pain, tingling, numbness and muscle weakness. Symptoms often start gradually and worsen over time. Spinal stenosis is most commonly caused by wear-and-tear changes in the spine related to osteoarthritis. In severe cases of spinal stenosis, doctors may recommend surgery to create additional space for the spinal cord or nerves. Most people with spinal stenosis are over the age of 50. There are two main types of spinal stenosis: 1. Cervical stenosis. where the narrowing occurs in your neck. 2. Lumbar stenosis where the narrowing occurs in the lower back.
Symptoms of spinal stenosis
Neck (cervical spine)
Numbness or tingling in a hand, arm, foot or leg
Weakness in a hand, arm, foot or leg
Problems with walking and balance
Neck pain
In severe cases, bowel or bladder dysfunction (urinary urgency and incontinence)
Lower back (lumbar spine)
Numbness or tingling in a foot or leg
Weakness in a foot or leg
Pain or cramping in one or both legs when you stand for long periods of time or when you walk, which usually eases when you bend forward or sit
Back pain
Causes of spinal stenosis
The backbone (spine) runs from your neck to your lower back. The bones of your spine form a spinal canal, which protects your spinal cord (nerves). Some people are born with a small spinal canal. But most spinal stenosis occurs when something happens to narrow the open space within the spine, such as the following :
Overgrowth of bone. Wear and tear damage from osteoarthritis on your spinal bones can prompt the formation of bone spurs, which can grow into the spinal canal.
Herniated disks. The soft cushions that act as shock absorbers between your vertebrae tend to dry out with age. Cracks in a disk’s exterior may allow some of the soft inner material to escape and press on the spinal cord or nerves.
Thickened ligaments. The tough cords that help hold the bones of your spine together can become stiff and thickened over time. These thickened ligaments can bulge into the spinal canal.
Tumors. Abnormal growths can form inside the spinal cord, within the membranes that cover the spinal cord or in the space between the spinal cord and vertebrae. These are uncommon and identifiable on spine imaging with an MRI or CT.
Spinal injuries. Car accidents and other trauma can cause dislocations or fractures of one or more vertebrae. Displaced bone from a spinal fracture may damage the contents of the spinal canal. Swelling of nearby tissue immediately after back surgery also can put pressure on the spinal cord or nerves.
In severe cases of spinal stenosis, doctors may recommend surgery to create additional space for the spinal cord or nerves.
Physio in Tralee specializing in the treatment of back pain, neck pain, foot pain and sports injuries.
Bunions
Bunions develop slowly. The big toe is made up of two joints. A bunion is a painful bony bump, also known as hallux valgus that develops on the inside of the foot at the big toe joint. Pressure on the big toe joint causes it to bend inwards towards the second toe. Over time, the normal structure of the joint changes, resulting in a bunion. The enlarged joint is often inflamed. The deformity gradually increases making it painful to wear shoes or walk. Bunions are more common in women. Many women wear tight, narrow shoes that squeeze the toes together. This makes it more likely for a bunion to develop. In most cases, bunion pain is relieved by wearing wider shoes with adequate toe room and using other simple treatments to reduce pressure on the big toe.
Bunion Progression
An advanced bunion can greatly alter the appearance of the foot. In severe bunions, the big toe may angle all the way under or over the second toe. Pressure from the big toe may force the second toe out of alignment, causing it to come in contact with the third toe. Calluses may develop where the toes rub against each other, causing additional discomfort and difficulty walking.
Foot Problems Related to Bunions
In some cases, an enlarged big toe joint may lead to bursitis, a painful condition in which the fluid-filled sac (bursa) that cushions the bone near the joint becomes inflamed. It may also lead to chronic pain and arthritis if the smooth articular cartilage that covers the joint becomes damaged from the joint not gliding smoothly.
Causes
Bunions may be caused by:
Wearing poorly fitting shoes—in particular, shoes with a narrow, pointed toe box that forces the toes into an unnatural position
Heredity—some people inherit feet that are more likely to develop bunions due to their shape and structure
Having an inflammatory condition, such as rheumatoid arthritis, or a neuromuscular condition, such as polio.
Diagnosis of bunions
Physical examination of bunions
Your doctor will ask you about your medical history, general health, and symptoms. He or she will perform a careful examination of your foot. Although your doctor will probably be able to diagnose your bunion based on your symptoms and on the appearance of your toe, he or she will also order an x-ray.
X-Rays
X-rays provide images of dense structures, such as bone. An x-ray will allow your doctor to check the alignment of your toes and look for damage to the MTP joint.
Nonsurgical treatment of bunions
In most cases, bunions are treated without surgery. Although nonsurgical treatment cannot actually “reverse” a bunion, it can help reduce pain and keep the bunion from worsening.
Changes in Footwear
In the vast majority of cases, bunion pain can be managed successfully by switching to shoes that fit properly and do not compress the toes.
Padding
Protective “bunion-shield” pads can help cushion the painful area over the bunion. Pads can be purchased at a drugstore or pharmacy. Be sure to test the pads for a short time period first; the size of the pad may increase the pressure on the bump. This could worsen your pain rather than reduce it.
Orthotics and Other Devices
Orthotics (custom-made shoe inserts) may be used to take pressure off your bunion. Toe spacers can also be placed between your toes to try and straighten the big toe. In some cases, a splint worn at night that places your big toe in a straighter position may help relieve pain.
Icing
Applying ice several times a day for 20 minutes at a time can help reduce swelling. Do not apply ice directly on your skin.
Medications
Nonsteroidal anti-inflammatory medications such as ibuprofen can help relieve pain and reduce swelling. Other medications can be prescribed to help pain and swelling in patients whose bunions are caused by arthritis.
Bunions and surgery
Your doctor may recommend surgery for a bunion, after a period of time, if you still have pain and difficulty walking despite changes in footwear and other nonsurgical treatments. Bunion surgery realigns bone, ligaments, tendons, and nerves so that the big toe can be brought back to its correct position.
Physiotherapists in Tralee stocking a wide range of orthotics to treat various foot conditions. Phone 0867700191
Equinus Foot Condition
The ankle joint connects the leg to the foot. It is formed by three separate bones, the tibia, fibula and talus. The shinbone (tibia) supports most of a person’s weight when standing. The outer bone (fibula) is the smaller bone of the lower leg. A small, irregular-shaped foot bone (talus) connects the tibia and fibula. Acting as a hinge, these bones form the ankle. The ankle joint allows movement such as walking, running and jumping, and also contributes to lower limb stability.
The ankle is reinforced by ligaments which connect bone to bone. Ligaments have a mildly elastic structure that allows them to stretch, within their limits, and then return to their normal positions. Ligaments protect the ankle from abnormal movements—especially twisting, turning and rolling of the foot.
Description
A person with equinus has a limited range of ankle motion and lacks the flexibility needed to bring the top of the foot upward, toward the shin. It may be either congenital or acquired, and occurs equally in both men and women. Equinus can be due to several different reasons including the following:
• bony block between the talus and distal tibia (osseous equinus);
• contracture or tightness of the soleus muscle (inner calf muscle);
• contracture or tightness of the soleus and gastrocnemius muscles (gastroc-soleal equinus);
• isolated tightness of the gastrocnemius muscles (outer calf muscle); and
• compensatory loss of ankle joint range of motion for some other condition such as pes cavus (pseudoequinus).
People with equinus often develop ways to compensate for their limited ankle motion. Depending on how a patient compensates for the inability to bend properly at the ankle, a variety of other foot conditions can develop, such as:
Plantar Fasciitis
Calf cramping
Achilles Tendinitis
Metatarsalgia (pain and/or callusing on the ball of the foot)
Flatfoot
Arthritis of the midfoot (middle area of the foot)
Pressure sores on the ball of the foot or the arch
Bunions and hammertoes
Ankle pain
Shin splints
Sesamoiditis
Hallux valgus
hallux rigidus
Hammer toes
Nonsurgical Treatment of Equinus
Some nonsurgical treatment strategies are aimed at relieving the symptoms and conditions associated with equinus. Treatment for the equinus itself may include one or more of the following options.
Heel lifts—Placing heel lifts inside the shoes or wearing shoes with a moderate heel may reduce symptoms by taking stress off the Achilles tendon and compensating for the restricted movement of the ankle joint. The joint is meant to have about fourteen degrees of movement ideally, so say it has only four degrees of movement, adding a ten degree heel lift helps compensate for the missing degrees of movement .
Arch supports or orthotic devices—Custom orthotic devices that fit into the shoe are often prescribed to ensure that weight is distributed properly, and to help control muscle/tendon imbalance. Again these devices will most likely include a heel lift.
Physical therapy—To help remedy muscle tightness, deep tissue massage of calf muscles along with a stretching program for the calf muscles are recommended.
For a quick simple video describing the condition click here


 Your spine is made up of lots of bones called vertebrae and discs stacked on top of one another, forming the spinal canal. The nerves of the spinal cord run down the length of the spinal canal. The discs in act like shock absorbers between the vertebrae. These discs are made of two components: a softer center (called nucleus pulposus) surrounded by a tough elastic-like band (called annulus fibrosus). A bulging disc is like a squashed jam doughnut before the jam bursts out. The disc sags and looks like it is bulging outward. With a herniated disc, the outer covering of the disc has a hole or tear. This causes the nucleus pulposus (jelly-like center of the disc) to leak into the spinal canal. It is like the jam leaking out from the inside of a squashed jam doughnut.
Your spine is made up of lots of bones called vertebrae and discs stacked on top of one another, forming the spinal canal. The nerves of the spinal cord run down the length of the spinal canal. The discs in act like shock absorbers between the vertebrae. These discs are made of two components: a softer center (called nucleus pulposus) surrounded by a tough elastic-like band (called annulus fibrosus). A bulging disc is like a squashed jam doughnut before the jam bursts out. The disc sags and looks like it is bulging outward. With a herniated disc, the outer covering of the disc has a hole or tear. This causes the nucleus pulposus (jelly-like center of the disc) to leak into the spinal canal. It is like the jam leaking out from the inside of a squashed jam doughnut.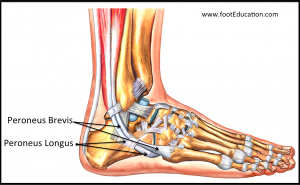 Peroneal tendonitis occurs when the peroneal tendons become inflamed. This happens when there is an increased load on and/or overuse of the tendons. This causes the tendons to thicken over time. If the injury becomes chronic, the tendinitis can progress to tendinosis. This is more serious and takes longer to treat.
Peroneal tendonitis occurs when the peroneal tendons become inflamed. This happens when there is an increased load on and/or overuse of the tendons. This causes the tendons to thicken over time. If the injury becomes chronic, the tendinitis can progress to tendinosis. This is more serious and takes longer to treat. cartilage can be damaged by injury or normal wear and tear.
cartilage can be damaged by injury or normal wear and tear. Dry Needling
Dry Needling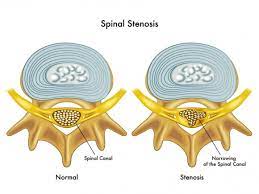 Spinal stenosis is a narrowing of the spaces within your spine, which can put pressure on the nerves that travel through the spine. Others may experience pain, tingling, numbness and muscle weakness. Symptoms often start gradually and worsen over time. Spinal stenosis is most commonly caused by wear-and-tear changes in the spine related to osteoarthritis. In severe cases of spinal stenosis, doctors may recommend surgery to create additional space for the spinal cord or nerves. Most people with spinal stenosis are over the age of 50. There are two main types of spinal stenosis: 1. Cervical stenosis. where the narrowing occurs in your neck. 2. Lumbar stenosis where the narrowing occurs in the lower back.
Spinal stenosis is a narrowing of the spaces within your spine, which can put pressure on the nerves that travel through the spine. Others may experience pain, tingling, numbness and muscle weakness. Symptoms often start gradually and worsen over time. Spinal stenosis is most commonly caused by wear-and-tear changes in the spine related to osteoarthritis. In severe cases of spinal stenosis, doctors may recommend surgery to create additional space for the spinal cord or nerves. Most people with spinal stenosis are over the age of 50. There are two main types of spinal stenosis: 1. Cervical stenosis. where the narrowing occurs in your neck. 2. Lumbar stenosis where the narrowing occurs in the lower back.