Arthritis – Rheumatoid vs Osteoarthritis
Rheumatoid arthritis
 Rheumatoid arthritis is a chronic inflammatory disorder that can affect more than just your joints. It is an autoimmune disease occurring when your immune system mistakenly attacks the synovium , the lining of the membranes that surround your joints. The resulting inflammation causes the synovium to thicken, eventually destroying the cartilage and bone within the joint. The tendons and ligaments holding the joint together also weaken and stretch. Gradually, the joint loses its shape and alignment.
Rheumatoid arthritis is a chronic inflammatory disorder that can affect more than just your joints. It is an autoimmune disease occurring when your immune system mistakenly attacks the synovium , the lining of the membranes that surround your joints. The resulting inflammation causes the synovium to thicken, eventually destroying the cartilage and bone within the joint. The tendons and ligaments holding the joint together also weaken and stretch. Gradually, the joint loses its shape and alignment.
It is unknown exactly what starts the process, although a genetic component appears likely. Newly developed medications have greatly improved treatment options. However, severe rheumatoid arthritis can still cause physical disabilities.
Symptoms
Signs and symptoms of rheumatoid arthritis may include:
- Tender, warm, swollen joints
- Joint stiffness that is usually worse in the mornings and after inactivity
- Fatigue, fever and weight loss
Early rheumatoid arthritis tends to affect your smaller joints first — particularly the joints of the fingers and toes. As the disease progresses, symptoms often spread to the wrists, knees, ankles, elbows, hips and shoulders. In most cases, symptoms occur in the same joints on both sides of your body.
Rheumatoid arthritis can also affect many non joint structures. This is the case in about 40 per cent of sufferers. These include:
- Skin
- Eyes
- Lungs
- Heart
- Kidneys
- Salivary glands
- Nerve tissue
- Bone marrow
- Blood vessels
Rheumatoid arthritis signs and symptoms can vary in severity and may come and go. Periods of increased disease activity, called flare ups, alternate with periods of relative remission — when the swelling and pain fade or disappear.
Risk factors
- Your sex : Women are more prone than men .
- Age : Can occur at any age, but most common between the ages of 40 and 60.
- Family history : Increased risk if there is a family history of the disease.
- Smoking : Cigarette smoking increases your risk of developing rheumatoid arthritis.
- Obesity: People who are overweight or obese appear to be at somewhat higher risk .
Diagnosis and Blood tests
People with rheumatoid arthritis often have an elevated erythrocyte sedimentation rate (ESR, or sed rate) or C-reactive protein (CRP), which may indicate the presence of an inflammatory process in the body. Other common blood tests look for rheumatoid factor and anti-cyclic citrullinated peptide (anti-CCP) antibodies. Rheumatoid arthritis can be difficult to diagnose in its early stages because the early signs and symptoms mimic those of many other diseases. There is no one blood test or physical finding alone that confirms diagnosis.
Imaging tests
Your doctor may recommend X-rays to help track the progression of rheumatoid arthritis in your joints over time. MRI and ultrasound tests can help your doctor judge the severity of the disease in your body.
Treatment
There is no cure for rheumatoid arthritis. Recent studies indicate that remission of symptoms is more likely when treatment begins early using medications known as disease-modifying antirheumatic drugs (DMARDs).
The types of medications recommended by your doctor will depend on the severity of your symptoms and how long you’ve had the rheumatoid arthritis. Medications used include :
- NSAIDs : Nonsteroidal anti-inflammatory drugs (NSAIDs) can relieve pain and reduce inflammation.
- Steroids : Corticosteroid medications, such as prednisone, reduce inflammation and pain and slow joint damage.
- Disease-modifying antirheumatic drugs (DMARDs) : These drugs can slow the progression of rheumatoid arthritis and save the joints and other tissues from permanent damage. Common DMARDs include methotrexate (Trexall, Otrexup, Rasuvo), leflunomide (Arava), hydroxychloroquine (Plaquenil) and sulfasalazine (Azulfidine).
- Biologic agents : Also known as biologic response modifiers. These are a newer class of DMARDs(Disease-modifying antirheumatic drugs) .These drugs can target parts of the immune system that trigger inflammation that causes joint and tissue damage. Biologic DMARDs are usually most effective when paired with a nonbiologic DMARD, such as methotrexate.
All the above drugs have side effects which need to be monitored.
Surgery
Medications can slow joint damage due to rheumatoid arthritis. When the damage becomes excessive surgery may need to be considered to repair the damaged joints.
Osteoarthritis
Osteoarthritis is the most common form of arthritis. It occurs when the cartilage that cushions the ends of bones in your joints gradually deteriorates. Cartilage is a firm, slippery tissue that permits nearly frictionless joint motion. In osteoarthritis, the smooth surface of the cartilage becomes roughed and worn. Eventually, if the cartilage wears down completely, you may be left with bone rubbing on bone. The disorder most commonly affects joints of the hands, knees, hips and spine.
Osteoarthritis symptoms can usually be effectively managed, although the underlying process cannot be reversed. Staying active, maintaining a healthy weight and other treatments may slow progression of the disease and help improve pain and joint function. When joint pain and damage is severe, doctors may suggest joint replacement surgery.
Symptoms
Osteoarthritis symptoms often develop slowly over time. Signs and symptoms may include:
- Pain. Your joint may hurt during or after movement.
- Tenderness. Your joint may feel tender when you apply light pressure to it.
- Stiffness. Joint stiffness may be most noticeable when you wake up in the morning or after a period of inactivity.
- Loss of flexibility. You may not be able to move your joint through its full range of motion.
- Grating sensation. You may hear or feel a grating sensation when you use the joint.
Risk factors
Factors that may increase your risk of osteoarthritis include:
- Older age. The risk of osteoarthritis increases with age as joints wear over time.
- Sex. Women are more likely to develop osteoarthritis, though it isn’t clear why.
- Obesity. Carrying extra body weight contributes to osteoarthritis in several ways, and the more you weigh, the greater your risk. Increased weight puts added stress on weight-bearing joints, such as your hips and knees. In addition, fat tissue produces proteins that may cause harmful inflammation in and around your joints.
- Joint injuries. Injuries, such as those that occur when playing sports or from an accident, may increase the risk of osteoarthritis.
- Certain occupations. If your job includes tasks that place repetitive stress on a particular joint, that joint may eventually develop osteoarthritis.
- Genetics. Some people inherit a tendency to develop osteoarthritis.
- Bone deformities. Some people are born with malformed joints or defective cartilage, which can increase the risk of osteoarthritis.
Summary
Rheumatoid arthritis is an auto-immune response where your body mistakenly attacks its own joints. Osteoarthritis is more or less due solely to wear on a particular joint over time.
Aside
Sometimes MRI results or Xray results state there is osteoarthritis present. With age most of us have some level of osteoarthritis due to wear on our joints. The important thing which your doctor will discuss with you is whether this level is normal for your age. A person can have mild osteoarthritis with no pain or symptoms and may have nothing to worry about.
Physiotherapist Tralee phone 086-7700191
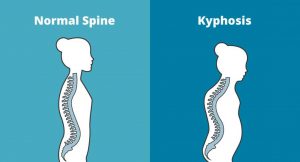 Kyphosis is an exaggerated, forward rounding of the back. It can occur at any age but is more common in older people. Age-related kyphosis is often due to weakness in the spinal bones that causes them to compress or crack. Other types of kyphosis can appear in infants or teens due to malformation of the spine or wedging of the spinal bones over time. Mild kyphosis causes few problems. Severe kyphosis can cause pain and be disfigurment. Treatment for kyphosis depends on your age, and both the cause and the effects of the curvature.
Kyphosis is an exaggerated, forward rounding of the back. It can occur at any age but is more common in older people. Age-related kyphosis is often due to weakness in the spinal bones that causes them to compress or crack. Other types of kyphosis can appear in infants or teens due to malformation of the spine or wedging of the spinal bones over time. Mild kyphosis causes few problems. Severe kyphosis can cause pain and be disfigurment. Treatment for kyphosis depends on your age, and both the cause and the effects of the curvature.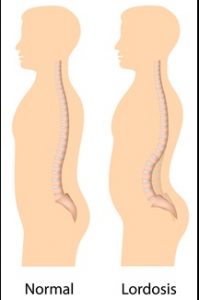 Some curvature in the lower back is normal. However, if your curve arches too far inward, it’s called lordosis, or swayback. Lordosis can affect your lower back and/or neck. The condition can lead to excess pressure on the spine, causing pain and discomfort. It can affect your ability to move if it’s severe and left untreated. Treatment of lordosis depends on how serious the curve is and how you got lordosis. There’s little medical concern if your lower back curve reverses itself when you bend forward. You can probably manage your condition with physical therapy and daily exercises.
Some curvature in the lower back is normal. However, if your curve arches too far inward, it’s called lordosis, or swayback. Lordosis can affect your lower back and/or neck. The condition can lead to excess pressure on the spine, causing pain and discomfort. It can affect your ability to move if it’s severe and left untreated. Treatment of lordosis depends on how serious the curve is and how you got lordosis. There’s little medical concern if your lower back curve reverses itself when you bend forward. You can probably manage your condition with physical therapy and daily exercises. Scoliosis is a medical condition in which a person’s spine curves sideways, usually in an “S” or “C” shape. In some, the degree of curvature remains stable, while in others, it increases over time. Mild scoliosis does not typically cause problems, however severe cases can interfere with breathing. The cause of most cases is unknown, but is believed to involve a combination of genetic and environmental factors. Diagnosis is confirmed by Xray. Treatment depends on the degree of curve, location, and cause.
Scoliosis is a medical condition in which a person’s spine curves sideways, usually in an “S” or “C” shape. In some, the degree of curvature remains stable, while in others, it increases over time. Mild scoliosis does not typically cause problems, however severe cases can interfere with breathing. The cause of most cases is unknown, but is believed to involve a combination of genetic and environmental factors. Diagnosis is confirmed by Xray. Treatment depends on the degree of curve, location, and cause.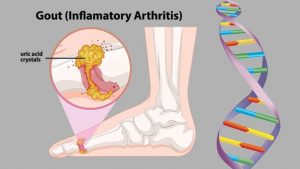 Gout is a form of arthritis which starts as a result of excess uric acid build-up in the blood, also called hyperuricemia. It is an extremely painful condition. Uric acid is produced in the body during the breakdown of purines – chemical compounds that are found in certain foods such as meat, poultry, and seafood. Normally, uric acid is dissolved in the blood and is excreted from the body in the urine via the kidneys. If too much uric acid is produced, it can build up and form needle-like crystals that trigger inflammation and pain in the joints and surrounding tissue. The condition often starts by affecting the joint at the base of the big toe. Attacks often occur without warning and in the middle of the night. They can come on quickly and keep returning over time, slowly damaging tissues in the region of the inflammation.
Gout is a form of arthritis which starts as a result of excess uric acid build-up in the blood, also called hyperuricemia. It is an extremely painful condition. Uric acid is produced in the body during the breakdown of purines – chemical compounds that are found in certain foods such as meat, poultry, and seafood. Normally, uric acid is dissolved in the blood and is excreted from the body in the urine via the kidneys. If too much uric acid is produced, it can build up and form needle-like crystals that trigger inflammation and pain in the joints and surrounding tissue. The condition often starts by affecting the joint at the base of the big toe. Attacks often occur without warning and in the middle of the night. They can come on quickly and keep returning over time, slowly damaging tissues in the region of the inflammation. Spinal stenosis is a narrowing of the space within the spine. This can put pressure on the nerves that travel through the spine. It occurs most often in the lower back and the neck. Some people are born with a congenital form, but most develop it as part of the degenerative cascade. Sometimes people do not feel effects of the narrowing, but as part of the aging process, most people will eventually notice radiating pain, weakness, and/or numbness secondary to the compression of the nerves or spinal cord. In lumbar stenosis, the spinal nerve roots in the lower back become compressed and this can produce – tingling, weakness or numbness that radiates from the low back and into the buttocks and legs, especially with activity.
Spinal stenosis is a narrowing of the space within the spine. This can put pressure on the nerves that travel through the spine. It occurs most often in the lower back and the neck. Some people are born with a congenital form, but most develop it as part of the degenerative cascade. Sometimes people do not feel effects of the narrowing, but as part of the aging process, most people will eventually notice radiating pain, weakness, and/or numbness secondary to the compression of the nerves or spinal cord. In lumbar stenosis, the spinal nerve roots in the lower back become compressed and this can produce – tingling, weakness or numbness that radiates from the low back and into the buttocks and legs, especially with activity.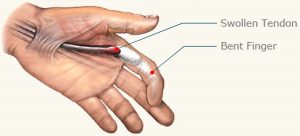 Trigger finger is a condition in which one of your fingers gets stuck in a bent position. Your finger may bend or straighten with a snap — like a trigger being pulled and released.
Trigger finger is a condition in which one of your fingers gets stuck in a bent position. Your finger may bend or straighten with a snap — like a trigger being pulled and released.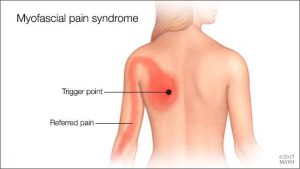 Myofascial Pain Syndrome
Myofascial Pain Syndrome
 Sub-acromial bursitis is a common cause of shoulder pain that is usually related to impingement of the bursa between the supraspinatus muscle tendon and the acromion bone(see diagram). Bursae(single = bursa) are fluid-filled sacs that help reduce friction wherever tendons move under or over bone. The Supraspinatus muscle runs along the top of the shoulder blade and inserts via the tendon onto the top of the arm(humerus bone). This muscle is used to lift the arm up sideways . Above the supraspinatus tendon and under the acromion there is a bursa. When this bursa gets inflamed and swollen it can become trapped under the acromium bone of the shoulder causing pain and inflammation.
Sub-acromial bursitis is a common cause of shoulder pain that is usually related to impingement of the bursa between the supraspinatus muscle tendon and the acromion bone(see diagram). Bursae(single = bursa) are fluid-filled sacs that help reduce friction wherever tendons move under or over bone. The Supraspinatus muscle runs along the top of the shoulder blade and inserts via the tendon onto the top of the arm(humerus bone). This muscle is used to lift the arm up sideways . Above the supraspinatus tendon and under the acromion there is a bursa. When this bursa gets inflamed and swollen it can become trapped under the acromium bone of the shoulder causing pain and inflammation.
 Instrument Assisted Soft Tissue Mobilization, also known as ”IASTM” for short is a process in which the clinician uses a set of ergonomically designed hand held instruments to break down the scar tissue and fascial restrictions in soft tissue (muscles, ligaments, tendons, and fascia ). The instruments you see in the photo are made of surgical grade stainless steel. Hypoallergenic aqueous cream or massage oil is used to facilitate gliding of the instrument along the muscle, tendon etc. during treatment. The technique itself is said to have evolved from a form of Traditional Chinese Medicine called Gua Sha. IASTM is a is a procedure that is growing rapidly in popularity due to both the effectiveness and efficiency 0f the technique.
Instrument Assisted Soft Tissue Mobilization, also known as ”IASTM” for short is a process in which the clinician uses a set of ergonomically designed hand held instruments to break down the scar tissue and fascial restrictions in soft tissue (muscles, ligaments, tendons, and fascia ). The instruments you see in the photo are made of surgical grade stainless steel. Hypoallergenic aqueous cream or massage oil is used to facilitate gliding of the instrument along the muscle, tendon etc. during treatment. The technique itself is said to have evolved from a form of Traditional Chinese Medicine called Gua Sha. IASTM is a is a procedure that is growing rapidly in popularity due to both the effectiveness and efficiency 0f the technique.